Last Updated: 08 October 2002
Phase 1
June 13, 2002
A broader perspective:
Pudendal,
Posterior Femoral Cutaneous
and its branch, the Inferior Cluneal Nerve
Disclaimer
I am not a doctor, and the following ideas are presented with no warranty, solely for the purpose of helping solving my sitting problem. If it also helps others I can only be happy. Please do give me your feedback and help me correct mistakes.
What others have to say
I only add this here to hopefully determine you to read once in detail this page.
Pay attention to the UPDATED Anatomy Charts, they will relate to you whether or not you have the same condition as I do!
1
That is a GREAT perspective Adrian! It's much easier to see where
things are with the (almost) 3D view. All the info is really useful,
will help a lot of people. Thanks again!
Randy
Conclusions First (if you want to know quick what this page is all about)
My Conclusion is that I may not need the surgery in the buttocks, nor the injections at the Ischial Spine, maybe not even in the Alcock' s Canal (which I am not so sure yet where it exactly is, but it appears to be farley close to the Ischial Spine - see pictures below to see why I am saying this).
How I injured myself
What I did
By extensive sitting, 16 hours a day for 6 weeks. I started having pain after 3 weeks, but I continued sitting.
I did this only because I was very frustrated with the fact I ended up having a large mortgage, while there were already a few unpaid things around. In parallel /addition we just had a small baby. As an aircraft engineer I have to be mobile, when a job ends in one place, the next job usually is in another city or even country. I knew I did not need a house in this circumstances. Yet somehow "w~life" has pushed me into having one.
Back then I only wanted to invest and improve in my professional skills, become some sort of Database Developer, Programmer or just a better Aircraft Engineer and eventually in parallel build a business of my own.
When about 8 months after buying that house I lost my job, and my wife shortly after me ( we used to work in the same plant) I have seen my worst previsions becoming a reality. Being a very calculated person, who rarely makes mistakes, and I have taken this trouble very seriously, and I overstretched /overworked myself, as described above.
After the injury I complained and suggested to doctors it could be nerve, blood vessel and/or scar tissue (fibrosis) but none came with any help. They told me is all in may head and that I should continue working. Being in financial trouble there was plenty of work and reason for concern around. A benign problem became over time a more chronic problem.
What I did not do
- I did not ride a bike for the last 10 years.
- I did not have any surgeries, cancer or infections in the area
- I did not do weight lifting, YOGA, or other strenuous exercises
- I do not have a history of a similar injury in my family
Why I may have a mistake in my diagnostic?
1. I self diagnosed myself.
2. Unfortunately I could not find a doctor (neurologist ?) to crosscheck my
thinking, in big part because of the huge waiting time (they make appointments
six month from now on), or because in the past I have been referred to other
specialties like CT Scan, MRI, etc which took a long time to get done and yielded
no conclusive results.
3. I am thankful to anyone who can give me feedback a.s.a.p because I have the
airplane to France in two days and I do not want to get that far for the wrong
reason.
What factors have let me to (wrongly?) believe that I have the Pudendal problem?
I jumped to think that I have the Pudendal problem because:
- When I have seen the Male Pudendal Nerve picture, because I have seen so may nerves there, and exactly or close to where my pain is, the first impression was that this would be the only nerves in the area, and that I finally found the reason for my trouble.
- Many people in the group claim pain in the same area like myself (apparently however we shall consider as well the Sir Henry Head zones) and Noci Receptors.
- I have not received any ideas from doctors in such a long time. Now I observed there is also another nerve in the same area (the Inferior Cluneal Nerve).
Nerves versus Blood Vessels, Fibrosis (?), etc
We shall also remember that not only nerves, but also blood vessels for
example may be affected, and apparently /possibly neurologists by definition do
not look into that, they just measure and treat nerves.
I learned that Rehumatologists by definition are concerned with "local modifications
of the tissue", a very broad range. If this will include local blood
circulations problems is not clear. I think I know that if a blood circulation
is closer to the surface, doctors recognize it by change in color of the skin.
I have no change in the color of my skin in my pain areas (see pictures
below).
How can we make sure nothing goes wrong for some in more "internal"
areas is not clear to me.
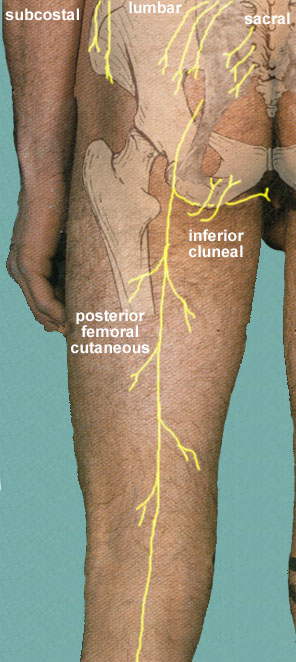
Inferior Cluneal Nerve
glutealregionlivingcutnerves_xxadrian_20020608_131248_rev___small.jpg
Source: http://mywebpages.comcast.net/wnor/glutealregion.htm
Posterior Femoral Cutaneous Nerve
Inferior Cluneal Nerve
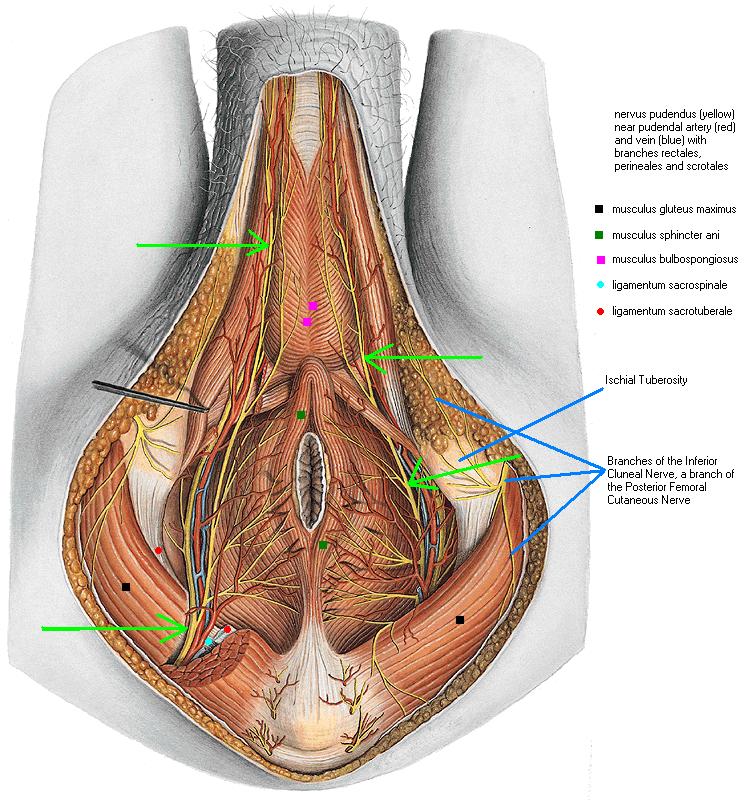
Male Pudendal Nerve
_xxadrian_20020509_122347_rev_A, MalePudendalNerve, Adrea, high res.jpg
Orig Source: Yahoo Pudendal Group
Ischial Tuberosity
Branches of the Inferior Cluneal Nerve, a branch of the Posterior Femoral Cutaneous Nerve
The nerve supply to the perineum
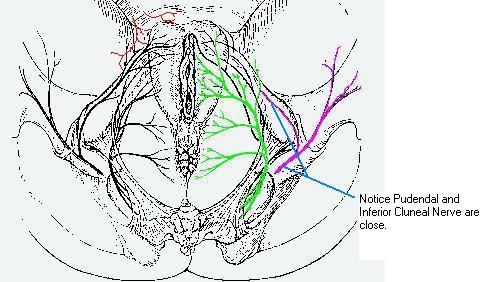
Java_Nerves_xxadrian_20020609_013137_rev_B.jpg
Source: http://www.manbit.com/oa/ go Subject /Anatomy /Pudendal Nerve Block /Figure 21.1
The nerve supply to the perineum originates from three main sources:
1. The Genito-femoral Nerve (L1,L2).
2. The pudendal nerve arises from the anterior rami of the second to fourth sacral roots. These form a trunk before leaving the pelvis via the greater sciatic foramen. It passes immediately behind the ischial spine and swings forward to enter the perineum via the lesser sciatic foramen. The nerve passes through the ischiorectal fossa where it gives off its terminal branches. The inferior rectal nerve innervates the external anal sphincter and the perianal skin. The perineal nerve innervates the sphincter urethrae and other muscles of the anterior compartment via a deep branch, and the skin of the perineum
posterior to the clitoris via its superficial branch. The dorsal nerve of the clitoris supplies the skin surrounding this structure.
3. The perineal branch of the posterior femoral nerve.
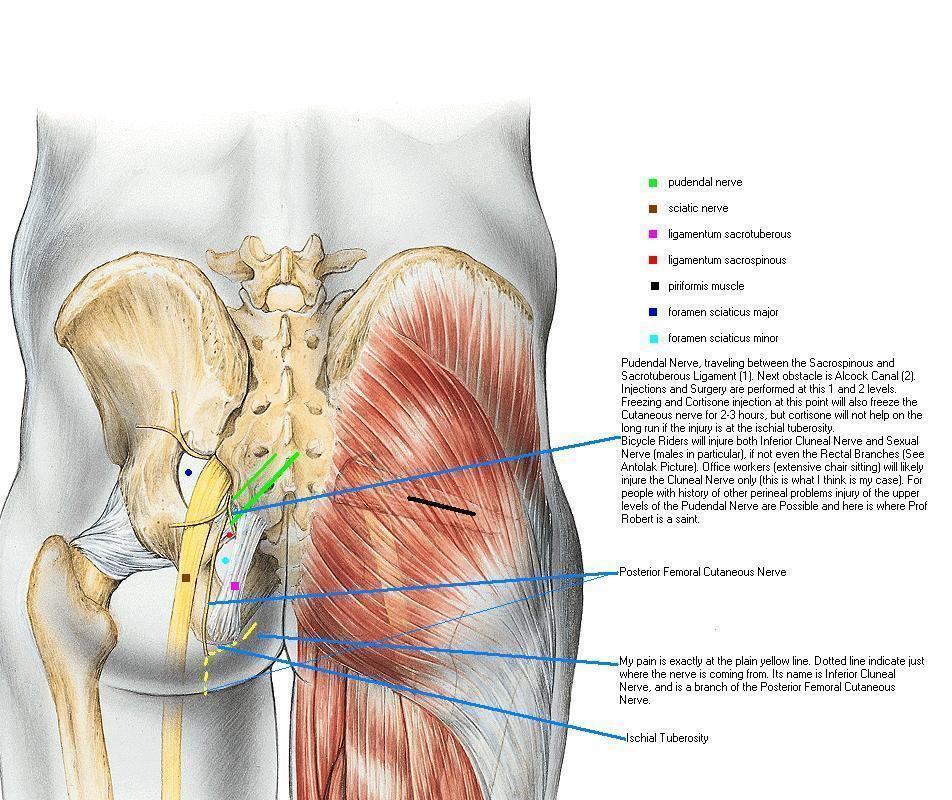
Pelvis 1 picture
__hr_pelvis1_xxadrian_20020501_124818_rev_A.htm
Orig Source: Yahoo Pudendal Group
Pudendal Nerve, traveling between the Sacrospinous and Sacrotuberous Ligament
(1). Next obstacle is Alcock Canal (2). Injections and Surgery are performed at
this 1 and 2 levels.
Freezing and Cortisone injection at this point will also freeze the Cutaneous
nerve for 2-3 hours, but cortisone will not help on the long run if the injury
is at the ischial tuberosity.
Bicycle Riders will injure both Inferior Cluneal Nerve and Sexual Nerve (males
in particular), if not even the Rectal Branches (See Antolak Picture). Office
workers (extensive chair sitting) will likely injure the Cluneal Nerve only
(this is what I think is my case). For people with history of other perineal
problems injury of the upper levels of the Pudendal Nerve are Possible and here
is where Prof Robert, Dr Bensignor, Dr Labat the rest of the team are by right
called "Saints".
Posterior Femoral Cutaneous Nerve
My pain is exactly at the plain yellow line. Dotted line indicate just where the
nerve is coming from. Its name is Inferior Cluneal Nerve, and is a branch of the
Posterior Femoral Cutaneous Nerve.
Dr Antolak, a new article (?)
antoart1_xxadrian_20020608_083923_rev_A, Notes.jpg
Source of this picture is http://www.prostatitis.org/antolakpudendal.html
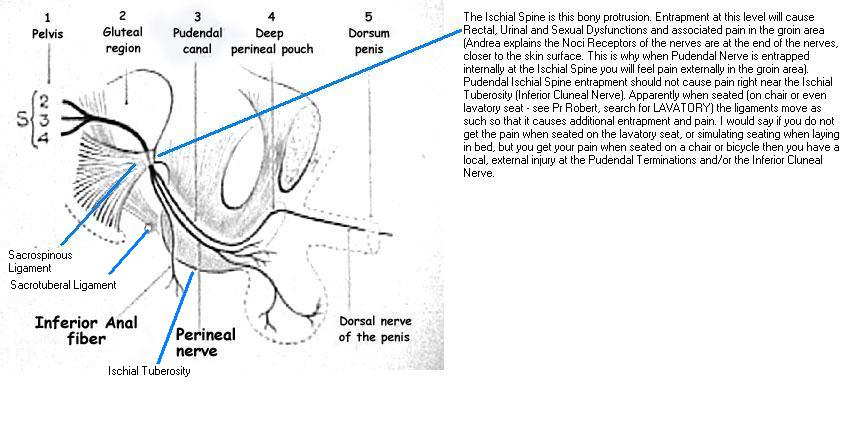
The Ischial Spine is this bony protrusion. Entrapment at this level will cause
Rectal, Urinal and Sexual Dysfunctions and associated pain in the groin area
(Andrea explains the Noci Receptors of the nerves are at the end of the nerves,
closer to the skin surface. This is why when Pudendal Nerve is entrapped
internally at the Ischial Spine you will feel pain externally in the groin area
).
Pudendal Ischial Spine entrapment should not cause pain right near the Ischial Tuberosity (Inferior Cluneal Nerve). Apparently when seated (on chair or even lavatory seat - see Pr Robert, search for LAVATORY) the ligaments move as such so that it causes additional entrapment and pain. I would say if you do not get the pain when seated on the lavatory seat, or simulating seating when laying in bed, but you get your pain when seated on a chair or bicycle then you have a local, external injury at the Pudendal Terminations and/or the Inferior Cluneal Nerve.
Sacrospinous Ligament
Sacrotuberous Ligament
Ischial Tuberosity
Pr Robert Article
Extract. Correct interpretation of the "lavatory" position referral required.
Clinical aspects
The site of the pain is in the perineum, and may be anterior (urogenital), posterior (anal) or mixed. Situated in the territory of the pudendal n., it is uni- or bilateral and to be distinguished from other regional pains with which it must not be confused (coccydynia, located more posteriorly, neuralgia of the ilioinguinal, iliohypogastric or genitofemoral nn.). In two-thirds of the cases women are affected. The character of the pain consists of sensations of burning, torsion or heaviness, and also of foreign bodies in the rectum or vagina. The pain is piercing and very comparable to acute toothache. The mode of onset is often gradual, but a fall is sometimes provocative; sometimes it is post-operative, especially after orthopedic procedures where a traction table has been used [3, 8]. Pain after repetitive energetic bicycling has led to the term "cyclist's syndrome" [1]. It may be much more indolent and develop gradually over time without a definite provoking factor. Lastly, it may be exacerbated by a regional surgical procedure: proctologic, urologic or gynecologic. The exacerbation of the pain is then only the patient's awareness of a therapeutic failure.
The positional nature of the pain is very suggestive. At a certain point in the case history the seated position provokes or exacerbates the pain. These patients have no pain at night and are comfortable when standing or lying on the non-painful side especially. It is an important point that they have no pain when on the
lavatory seat, ie when the painful zone is relieved from pressure. The main daily activities requiring the seated position (work, meals, driving, theaters, etc) are no longer available to these patients, whose mental attitude is one of chronic pain sufferers so obsessed with their miserable state as to be rapidly regarded by their doctors as psychiatric cases.
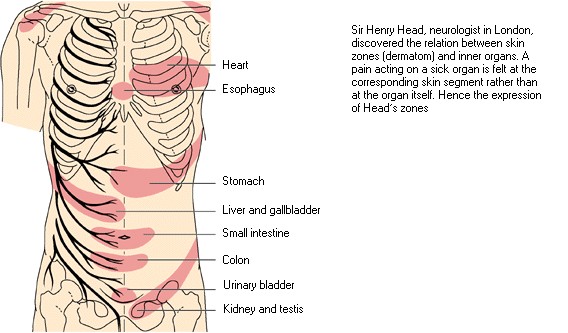
Sir Henry Head zones
Head's zones_xxadrian_20020501_130135_rev_A.jpg
Orig Source: Yahoo Pudendal Group
Sir Henry Head, neurologist in London, discovered the relation between skin zones (dermatom) and inner organs. A pain acting on a sick organ is felt at the corresponding skin segment rather then at the organ itself. Hence the expression Head's zones.
Pelvis 4 picture

pelvis4_Alcock_Canal_xxadrian_20020501_125355_rev_A.jpg
Orig Source: Yahoo Pudendal Group
It is being said that Alcock' s Canal is short, by no means as long as the Probe. Ref as well to the Male Pudendal nerve, how the nerve appears from under the muscle and Sacrotuberous ligament. More clarification is required as of what exactly the Alcock' s canal actually is.
Surgery Cuts

Surgery_Cuts_xxadrian_20020608_233355_rev__.jpg
Orig Source: Yahoo Pudendal Group
Injections are being made close to the middle of this surgery cuts (and it shall be no surprise, because both injections and surgery target the same spot ...!)
I honestly believe I do not need this surgery, nor injections at this level, but rater directly where I have marked up below.
My Pain Patterns
Cortisone is Good

Notice how my marks my coincide with one of the branches going up of the Inferior Cluneal Nerve.
Some of the Pudendal Branches might be affected as well, but I do not have any Rectal, Urinary, Penile, Sexual pain or malfunction.
I am convinced that if I need cortisone, I need it locally, as the picture indicates.
Residual Pain Area

Residual Pain Area.jpg
Cortisone applied locally permanently relived 60-70 % of my pain. Doctor declined to inject more in-between the legs for concern of unknown territory.
Note: My markups are not perfect, as I had a hard time accurately marking myself. I may be to high, or this is how it was that day. More recent picture shows marks a lot lower.