Last Updated: 07 October 2002
Phase 2
June 25, 2002
Note: This page has been written at a very late hour, and I will not have soon time or opportunity to revise it. Please take it "as is".
Dr Watling (Neurologist) - London /Ontario/Canada
I have met Dr Watling just two days before I departed to FRANCE. At that time my tickets were length ordered and paid for. He agreed I possibly have Pudendal Nerve problems, he indicated that he does not have direct experience with this particular problem, he suggested that he can indicate certain medications, and as a general tip in regards to my trip to France recommended to be cautious in regards to aggressive (surgical...) interventions at this time.
Departure for France did not come easy
The next day after the above appointment, upon my suggestion, Greg provided us with pictures of the surgery cuts. I have been shocked by this new information, as I was always thinking that if it must be surgery, it shall be closer to directly where my pain is. I was disappointed that none of the conversations I had with my doctors prepared me in any way for what I was actually seeing. Considering my latest exposure and experiences, the only thing I am sure about today is that I still know and understand too little about the complexity of my problem.
{kind=link}
However, I left in the hope and expectation that Dr Bensignor has the experience
and willingness to treat all sorts of traumas in the area, including such
problems in and around the ischial tuberosity. In cooperation with Dr Labat (PNMLT)
he managed indeed to at least get me closer to a diagnostic. It was for me high
time to do some real action since back home in Canada I had difficulties lately in finding a doctor to do or
suggest something of practical value for my problem. In general was effectively
impossible to find a doctor knowledgeable and willing to inject or do something about this
area. Dr Bensignor stated in an email or conversation that after surgery some
patients still have some left over pain in this area, and they treat it with local injections.
In regards to my departure for France I shall express here my gratitude to the Yahoo Pudendal Group active
members for effectively helping and guiding me in this journey.
France Visit 1
Dr Labat has performed the Latency Test June 13, 2002 at 10:00 (250 EURO)..
The same day at 15:30 Dr Bensignor performed an injection with anesthetic and
cortisone internally, at the level of the Ischial Spine (250 EURO).
Dr Labat - Nantes /France
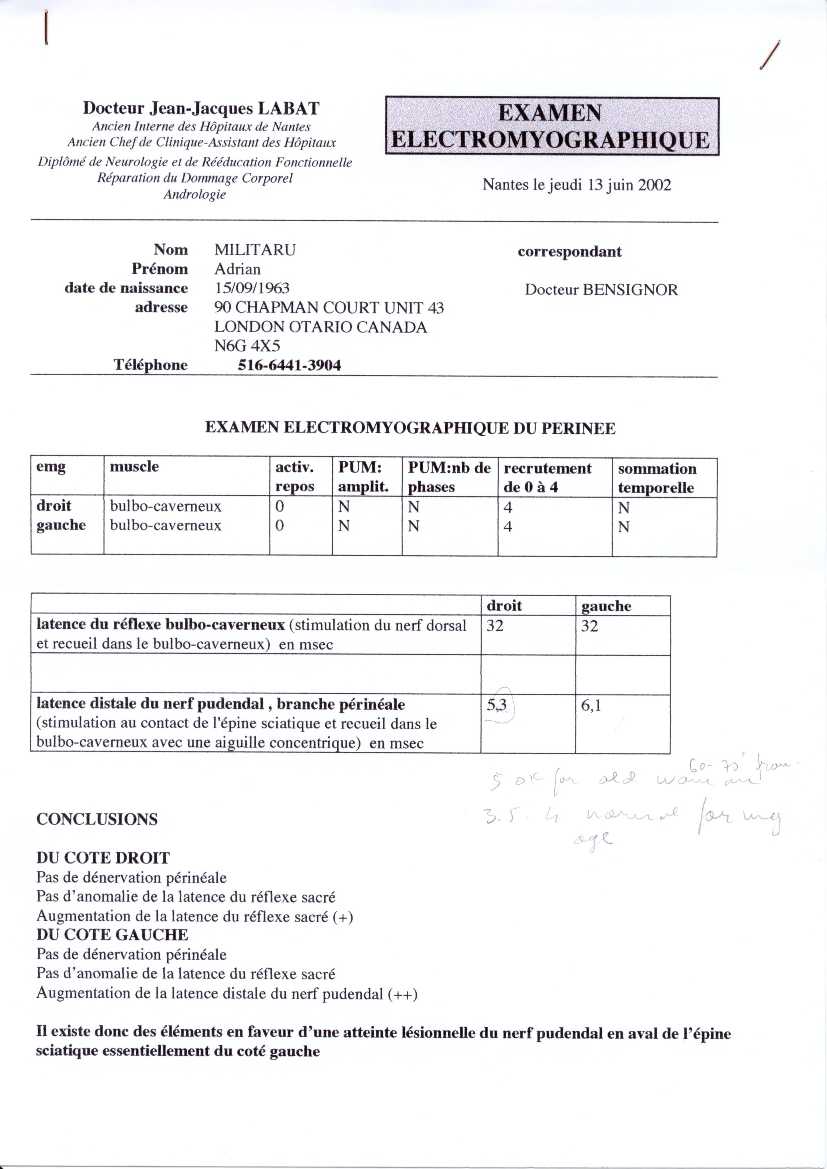
If you refer to picture of Dr Antolak, the test is performed as follows::
{kind=link}
Patient lies on his back, knees flexed, legs open apart. Needle is inserted just under the skin underneath testicles, a bit to the side from center, and doctor asks you to squeeze your rectum. When needle is properly placed, you will hear a sound in the computer. Keeping the needle inserted, a piece of metal is held by hand on the upper side of the penis (no , it does not need to be erected...) and measurement is performed. Then a finger wrapped in some computer like copper flat band is inserted in the rectum, and measurement is done once again. When you look on the picture you can understand how the nerves circuitry is tested. Then needle is inserted the other side and procedure is repeated.
I had some pain when Dr Labat was pushing downwards on my rectum. He said this is not normal. I normally do not have pain at defecation, or else, I did have some hemorrhoids, 10 years ago well treated for good with sclerosant injections, but Dr Labat did not agree that this might be the cause.
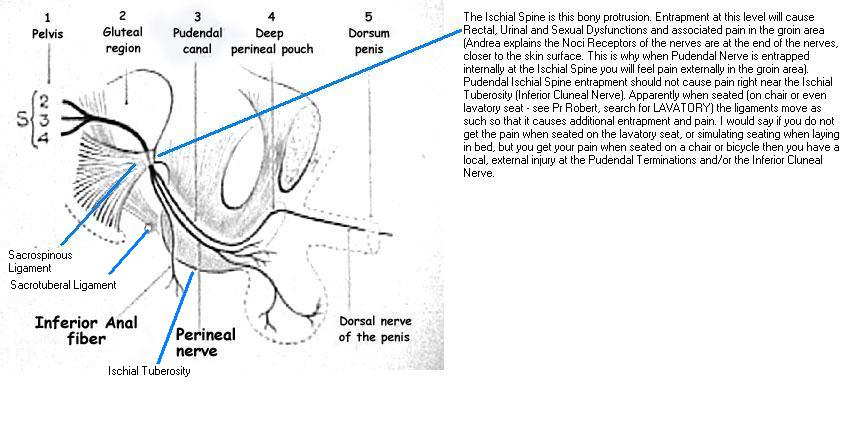
In my current understanding one can have entrapment at the level of the ischial spine (internally between the sacro-spinous and the sacro-tuberous ligament) or can have affection of the terminal branches of the nerves. If any, I assume I may have some inflammation of the terminal rectal branches.
On a pain scale from 0 to 10, I asses a pain level of 4 or 5 for the procedure, and is only momentary, nothing to worry about.
Dr Bensignor - Nantes /France
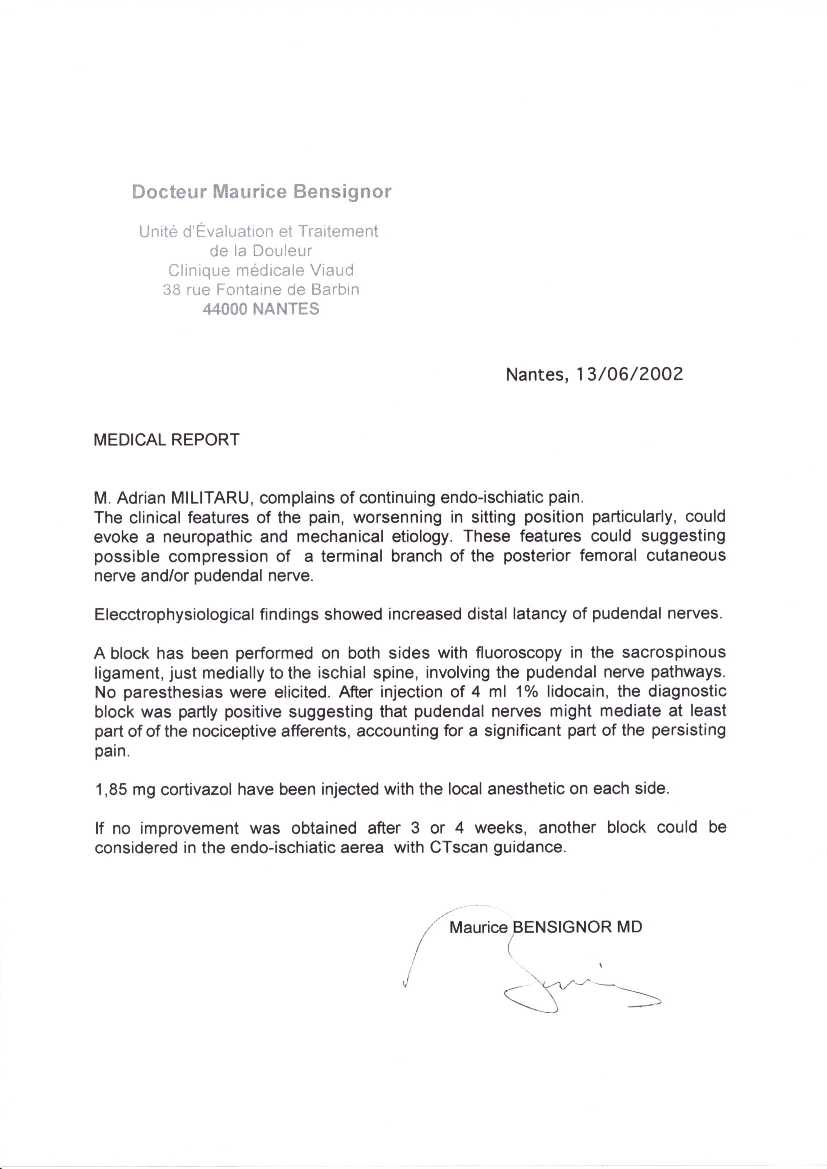
Dr Bensignor Report (alternatively Right-Click and save target, then view with MS Photo Editor or print)
We discussed the issue that I assume I have more local overuse injury. To exclude internal PNE we proceeded with the standard injection at the level of the ischial spine. I experienced 30 min 70% relief of my pain.
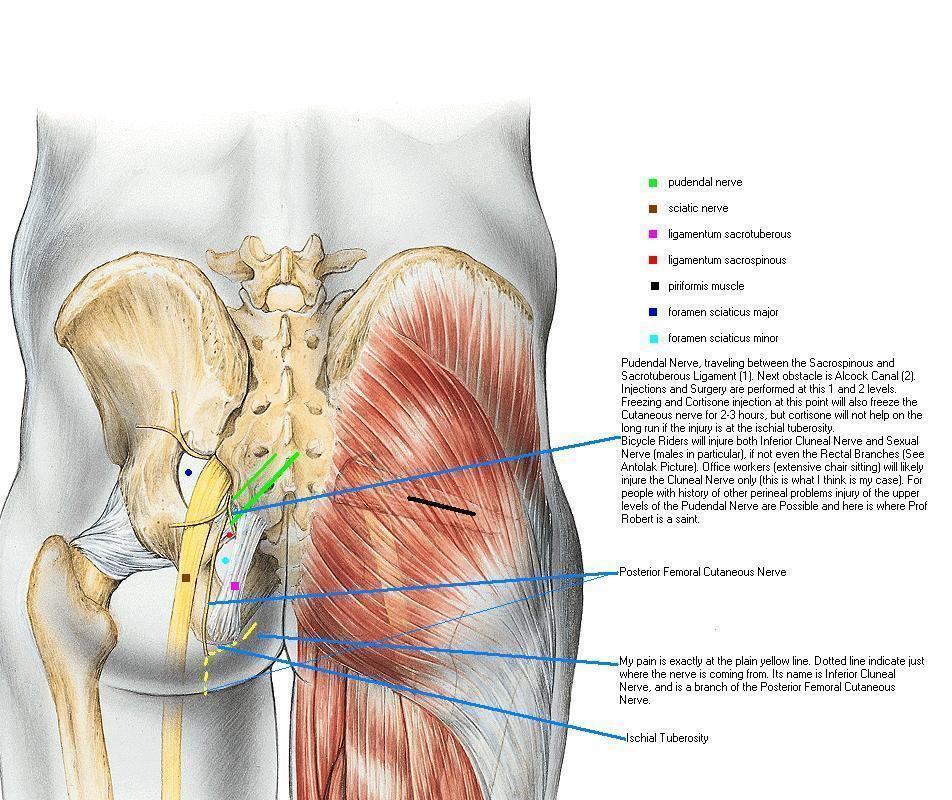
We discussed the aspect that in picture Pelvis 1 the coetaneous nerve should not be frozen as well. Dr Bensignor explained that in 3D they are really far apart, and it will be no problem.
{kind=link}
Unfortunately subsequent the injection I had some pain on the right side (while I had absolutely no pain on the left side), in particular when lifting my knee. Luckily it disappeared after about a week.
Dr Bensignor was willing to go with me the same night at the CT Scan and also perform local injections in and around the Ischial Tuberosity. We then again agreed to allow the first injection three weeks, so that in case of positive effects, we do not get confused as of which one was beneficial. We agreed I shall come June 4, 2002 at 19:30, when the scanner in hospital is available, for local injections, in and around the ischial tuberosities.
Dr Fanai (Neurologist) - Wiesbaden/Germany
He can perform the Latency test, but by right felt is no need to repeat it.
He basically suggested that I have more a Tennis Elbow like condition at the point where the ligaments and tendons attach to the ischial tuberosity, and encouraged me to go back to Dr Bensignor, as he himself does not perform such injections.
Below is a quick copy and paste from Word file _xxAdrian_20020627_173000_Rev_B, Dr Fanai, Appointment 01.doc.
1.
Contact Info
Dr Fanai Münsterman, Neurologist,
Tel: 0611-9003890
Luissenstraße 18
Wiesbaden, Germany
I
understand that he has (some?) experience with the Pudendal Nerve and for sure
he can perform the Motor Latency Test for the Pudendal
Nerve (Very few doctors can do this at all!). He said that since I already have it done by Dr Labat, it does not make sense for him to repeat it. He did
have a variety of neurological electrical measurement instruments in his praxis.
Unfortunately he does not perform himself cortisone infiltration’s (which is
another word for injections).
2.
Medical and Conversation Report
I have
made my presentation which included:
·
how the injury
occurred by super extensive and super intensive sitting for six weeks
·
The fact
Cortisone injection in the tip of Ischial Tuberosity was 60-70% effective with
permanent lasting results, but also that the doctor who performed it declined to
perform more then one round of it and more in-between the legs, for fear of
unknown territory and nerves, etc
·
The Pudendal
Anatomy Charts and what the doctors in France do, the fact Dr Bensignor injected
anesthetic and cortisone at the level of the Ischial Spine, where the anesthetic
froze for 30 min 70% of my pain, but no improvement happened in two weeks after
the injection.
·
The fact I do
not think I have entrapment internally at the Ischial Spine, but I think I
require local treatment at the level of the Ischial Tuberosities
·
The fact that I
have tried to avoid sitting for weeks and months in a row which helped for the
moment, and tried different exercises, but it did not help solve the problem on
the long run and therefore I think I require some external help in order to get
out of this situation.
He
checked me out, and pushed with the finger around until pain was triggered.
Subsequently
he expressed following opinions:
The
bottom line of his opinion is that I do not have so much nerve irritation
problem, but rather an untreated Tennis Elbow like situation (an inflammation of
the insertion of various ligaments in and around the Ischial Tuberosity). He
concludes this by the fact that cortisone was so effective for me in the past,
and if I were to suffer from major local branches nerve damage or irritation,
cortisone would not have been so effective. (Dr Salup also expressed the opinion
that if it is real nerve damage in some cases you may recover, in others you
will not recover – thus skepticism in relation to healing nerves through
cortisone ?!?)
He
indicated medication ZOLOFT 50 mg for six months once a day in the morning.
Effectiveness to be expected within a week, normally in three weeks, etc.
He
explained that hand movement for example is controlled by a small area on the
brain. For a pianist or violinist the same area becomes almost three times lager
in diameter. Same thing happens with chronic pain, just that with chronic pain
you want to forget /unlearn the brain as fast as possible about the old pattern
of pain, in particular after the original cause if genuine pain has been cured
or eliminated.
3.
What Dr Fanai recommended
·
Perform
more local cortisone injections to clear the inflammation. Do more of them and
more precisely placed.
(Naturally do not exceed the max recommended dose or frequency, so that no
tendon /ligament rupture occurs – Adr).
·
Naturally avoid
sitting and stenos exercises (same like in Tennis elbow, etc)
·
Take
medication to help brain unlearn the pain pattern, in particular after the original cause of pain has been eliminated
(ZOLOFT 50 mg one per day in the morning for six months).
4.
Open Questions
4.1.
Bone Scan
I have had bone scan done
in
Canada, and the result
was negative.
As far as
Bursitis is concerned, Ultrasound Imaging did not show any liquid accumulation
in the ischial bursas, and therefore Ischial Bursitis has been eliminated. Yet
again, I believe at least some minor disturbance of the bursas must be present
and part of the problem. According to Mayo Clinic Book, bursitis is treated
as well with Cortisone.
4.2.
Abnormal Motor Latency Test values
In this new perspective what is then the meaning of the Latency Test abnormal values of the Rectal Branch of the Pudendal Nerve Dr Labat performed? I can only say to this that I have read reports from patients operated by Pr Robert in French, when some people had absolute normal measurements but because they had such great pain, the decision for operation was taken and PNE was found and addressed with good results. One suggested explanation is that when entrapment is rather punctual it will cause pain but not delay the signal, etc
4.3.
What about the burning pain, which seems typical for nerve irritation
pain, and pinching /stabbing pain when walking (after recent prolonged/forced
sitting)?
·
Could it be
simply an exacerbation /accumulation of pain caused by the same tennis Elbow
like problem?
·
Could it be
perhaps the brain over-reaction he explained about?
·
Could it be
still some incipient form of local nerve injury?
5.
Other Conclusions and Observations
5.1.
A chair (as opposite to a bicycle saddle?) should be unlikely to cause
injury to major local nerve branches. We do not sit on nerve branches, not even
for a minute, that’s for sure in my mind
I have
never seen a good 3D image of where exactly the Pudendal and Coetaneous nerves
run, but I now tend to believe that since I only seat on a regular, upholstered
office chair, it should be very unlikely to have directly injured the passage of
the major local branches. I would have considered this more of a possibility if
I would have used a bicycle as cause of my injury, but this is not the case.
On the
other hand Jack has
brought to my attention that while we do not seat directly on nerves, they may
get compressed by muscles, tendons, ligaments and fat, etc when we sit. =>I
do not know what conclusion to draw anymore.
5.2.
Freezing the Pudendal nerve is not an automatic conclusion!
If pain disappears when freezing the Pudendal and/or the Coetaneous nerve it is an indication that the particular nerve has an injury an generates the pain only when all other causes have been eliminated (like cancer, osteoporosis, etc). However Bone Scan was normal so Tennis Elbow does not seem the problem, and Bursitis has been eliminated by ultrasound test. Possibly low level leftovers of such affections to continue bothering me?