Last Updated: 16 October 2002
Phase 3
July 4, 2002
Foreword
I sincerely hope by sharing with you the details of my experience, it will help those who have not had it yet, and in the same time, by becoming a more informed patient, save some hassle those who treat you. I wished I knew more before I started, since as you will find out /read below, my lack of correct understanding could have caused some problems to myself, be it by simply hindering the doctor to do his job correctly.
For those who have not had the time to read the entire site I shall state here again the beginning note of this site, and that is that I feel quite dissatisfied with the way the material is presented, and even more I would have preferred not to be in the position to need to do it, but since it tries to serve the practical purpose of helping us get better, I have to go ahead with it just the way it is.
Dr Bensignor Report, Visit 2, July 4, 2002
> Nantes, 04/07/2002
>
>
> M. Adrian MILITARU complains from chronic perineal and prominantly
> endoischiatic pain. The pain is worse sitting and partially resolves in
> decubitus, in the morning or sitting on the toilets.
>
> Electophysiological explorations showed an increased pudendal nerve distal
> latency.
>
> All this features match with the diagnosis of pudendal neuropathic pain
> possibly originating in a nerve-ligament conflict or in an irritation of
> pudendal nerve in its endo ischiatic pathway, near the insertion of
tendons,
> with possible local inflammation.
>
> A therapeutic block was performed in Alcock's canal, in its endoischiatic
> pathway under CT scan control with 3,75 mg cortivazol and 8 ml 1 %
> lidocaine. The diagnostic block was positive.
>
>
>
>
Maurice F. BENSIGNOR MD
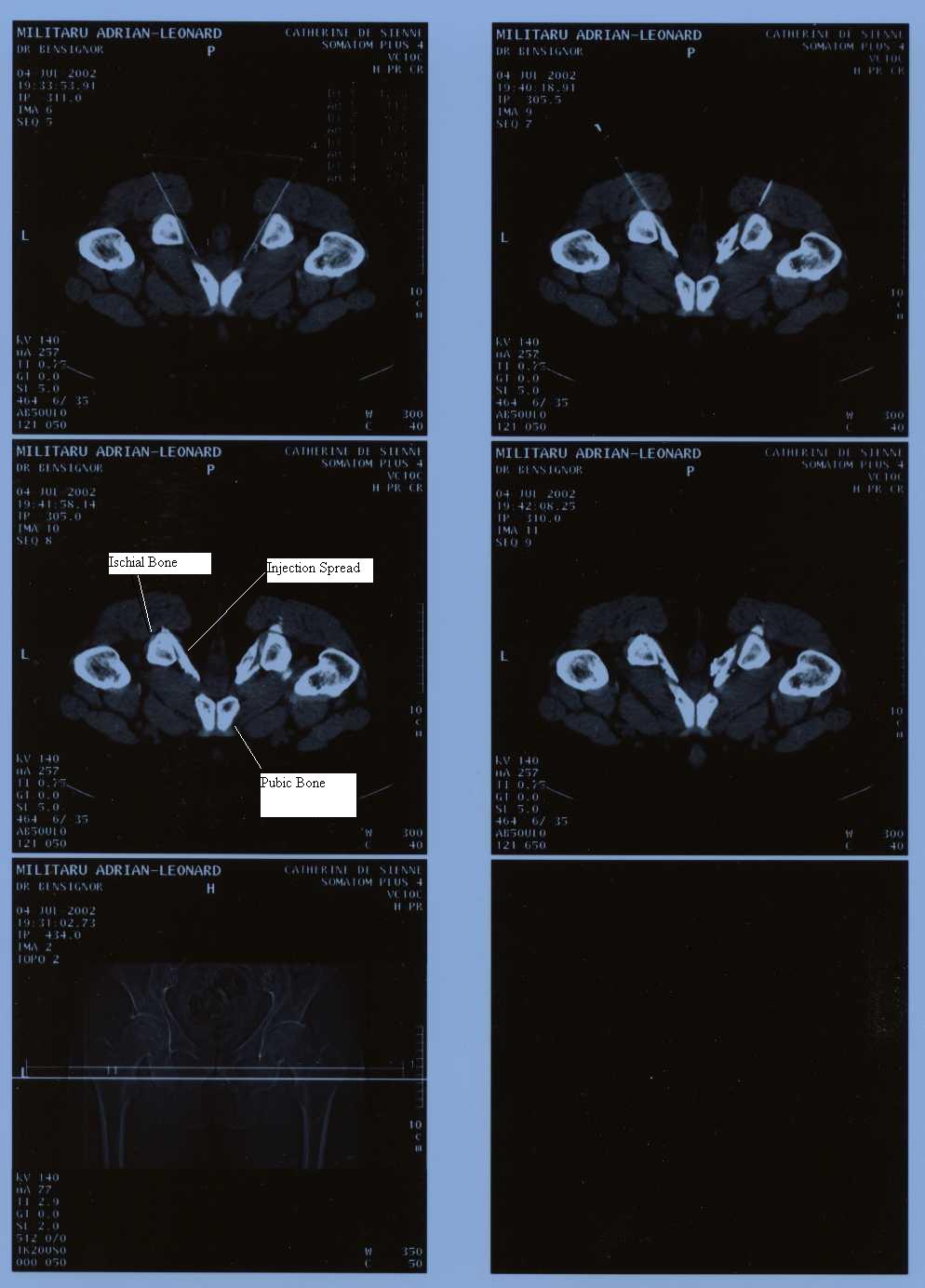
Infiltration CT Scan Image (_xxAdrian_20020711_143000_Rev__web.jpg)
Knowing my experience may help you behave better. Stay still during injection procedure!
Considering the location description I gave to my pain as described throughout this web, after at the first visit we injected internally at the Ischial Spine with no improvement, I was expecting really local injections in and around the Ischial Tuberosity, similar to those shown in Cortisone_is_Good.jpg.
{kind=link}
I am not sure how, but I was expecting to lay on my back, legs open, knees up, just as in above picture.
Now I was in the CT ring, 100% horizontal, face down. When Dr Bensignor started to disinfect with alcohol on my buttocks, I grew very impatient, as I thought we will not be doing the right spot.
When I started moving and turning, Dr Bensignor got nervous "What's wrong with you, stay still, this is 1 mm precision work I am doing here". I gave up any opposition. and went on with my fate. He finished inserting the needles. I was pleasantly surprised to have no pain while he was doing that. He did CT verification and said the needles are set perfectly. This was a comforting news for me, as now I was concerned that because of my moving we will not be able to do the right thing. The injection liquid was introduced.
Here is where the wondrous thing begun. I started to feel that the normal pattern of my pain is directly addressed. When first started, my pain felt like an elongated painful fiber, especially on the left side. Now the injection activated exactly that area, exactly that elongated fiber. In other words, the injured areas as opposite to the more healthy areas were responding with prevalence.
Once out of the CT, Dr Bensignor asked me to sit. He came to me with the CT picture above, and helped me understand it. Long needles have been inserted just beside the inside of the Ischial Tuberosity (exactly what I wanted according to my initial preparation and understanding) but almost up to the pubic bone, so a lot more has been addressed, and a "long" injection was performed. I was thrilled with joy. I thanked him dearly, and explained that I grew concerned just because so many other doctors have failed to help me before. In return he was happy as well for my joy and hopefulness.
Nobody I have seen before was even remotely capable or willing to perform such an in my view record braking action /injection. I encourage everyone who needs it to go for the best.
What to expect after the injection
That night I was really happy, I felt like highly celebrating.
For two days I had no pain at all, which hinted to a very well done injection and an encouraging thing if I had to do it again. I extended my stay to ask Dr Bensignor if it is anything else we could do at this time, but I found out he went in vacation for a week. I phoned Dr Robert's office, and I was thrilled to have the chance to speak to him personally for the first time. I guess he was available mainly because it was a post intervention question. He explained me that the procedure I have received is an injection in the Alcock' Canal, the injected cortisone is a very powerful substance, and that I will experience some mild exacerbation of my pain (which indeed started building up after two days or so and I feel it as I am writing this). He further told me we now have to wait for three three weeks for the medication to make its effect, and is nothing further can or should be done at this time. With this new knowledge, I thanked him for his intervention, and took my mind off of the medical subject, happy in having quite successfully completed this step I was waiting for so long.
As I had two more days until my airplane to Germany, where I have campus at my sister for the duration between interventions, for the next two days I went on the Nantes Atlantic beaches, in the pleasant company of a fellow from my room.
Is now to early to say that I have solved my problem, but so far I am extremely pleased that finally something of practical value has been done again, in particular because cortisone has helped me so much in the past (60-70% permanent resolution of my problem). I will keep you posted as things evolve.
Related Emails
Dr Bensignor email replay to the Group
> 1) One lady, (she's on your spreadsheet) lives in Canada.
> She's talking with someone who wants to do a pudendal nerve block
on her, > but to go through the vagina. Will she be able to hit the
right
place > (ischial spine) through the vagina?
It is theorically possible to reach the iscial spine through a trans
vaginal
approach. The operator has to be very skillfull though and should use
a
special needle. Many gynecologists perform trans vaginal pudendal
nerve
blocks, mostly for obstetrical purposes. They generally use a special
needle
designed to prevent a deep injection. This technique is appropriate to
obtain a local anaesthesia of the cervix. It is doubtfull that it
could
allows to reach the posterior ligaments or the falciformis process of
the
sacrotuberous ligament accuratly. I would say such a block could have
a
diagnostic value in case of anterior (genito-urinary) pain, but not
for
posterior (anorectal) pain. A long term therapeutic effect from
steroids
through that route is unlikely.
>
> 2) for the people > who are cured through shots alone, are they cured immediately or does it > come gradually? Are a series of blocks done?
There is generally an immediate but short (a few hours) effect of
local
anaesthetics. In good cases, the relief from steroids takes 2 to 4
weeks,
sometimes after a transcient worsenig of the pain for a few days.
Long term
relief usually requires 2 or 3 injections. When a long term (several
months)
relief is obtained from these injections, a recurrence of the pain may
happen but is exceptionnal (less than 10%).
Post Injection Pain Description
I am very behind with the group messages.
I guess in a month I have hundreds to read.
I wanted to paste/cc this message to the group, but right today it gives me some
yahooo server error.
I really want to to get back to all those who helped me with last minute
information before my departure.
----- Original Message -----
From: "Jack Harich" <[email protected]>
To: "Mariana Daian" <[email protected]>
Sent: Wednesday, July 10, 2002 7:50 PM
Subject: Re: Fw: Medical report
> Andrian,
*Adrian
Thanks for the report and images. It looks like they inject much more at
Alcock's canal than at the ischial spine. Looking at your reports, it was
twice as much for the cortivazol and lidocaine.
*nice observation, I did not think or had time to compare. I guess is simply
because is a long injection.
>
> Did Dr. Bensignor inject inside the canal or on a nearby ligament?
*I think is part parallel with some nerve branches (at the deeper end ?),
part parallel/close to Alcock's Canal (which is 1-3 cm short) and the most
superficial part was in the ligaments attached to the ischial tuberosity (on
the left side the injection was longer, but luckily is also the worse side
of mine.). Since the nerve should not be touched, I guess the injection is
in the walls of the canal, but on which side of it and how I do not know,
this is why I suggested long time ago we should get better at 3D Anatomy.
unfortunately my "work conditions" here are difficult, and the
computer very
slow, really slow at some actions, etc. Also my pain is now a bit greater
even without sitting.
>
> Did 100% of your pain go away for a short while?
*yes, for the entire evening I would say. I never tried to sit on it, except
right after the injection when Dr Bensignor asked me to, and I told him I
think he hit very well the problem area, and thanked him very dearly.
However now in day 5 or so, I see more and more pain, without actually
sitting on it, but it feels like a good, healing pain. I have been told by
Pr Robert, and also recent email from Dr Bensignor via Greg says that this
is what that will normally happen. This is good, that means the injection
stuff really works, is not like water. Pr Robert said "this is very
powerful substance", and indeed it seems it is.
I hope that after some time the new pain will start to regress, and see some
healing after it.
What I like the most is that the "new pain" seems to mold/emulate
exactly
the pattern of the old pain, shape and for example more on left then on the
right, etc
let me know if you can better document with 3D pictures where the nerves are
and where the injection was placed. I am just so curious.
>
> I hope the steroids have a beneficial long term effect.
>
> Good luck,
>
> Jack
>
>
> Mariana Daian wrote:
> >
> > Dear Jack,
> >
> > Dr Bensignor sent my report per email at home. I just received it
myself
from
> > my wife. Regards, Adrian.
Andrea re Alcock Canal Injection
By some US-people I have heard that their docs
sometimes hit the nerve itself and therefore they climed the wall at the
practice office - for this I have asked Bensignor to please be careful, but he
said he would have much more experience and that it won't happen with him. So I
think you really get the shot into the Canal, for this speaks also the large
white "fields" in pic # 2, after the liquids were injected.
In the end I suppose you are now convinced that it's not necessary to be treated
exactly where your pain is!
=> Yes, Andrea, you were right, I still have to learn and understand.