|
1. Anton, R., "A Common Sense Approach to Diagnostic Imaging of Carotid Vascular Disease", Applied Radiology, July 1997.
2. Schmalfuss, I., "Noninvasive imaging of carotid artery stenosis", Applied Radiology, April 1998.
3. Kelley, R., "Stroke prevention and intervention; New options for improved outcomes", Postgraduate Medicine, February 1998.
4. Merck Research Laboratories, The Merck Manual of Diagnosis and Therapy, 17th Ed., 1999
5. Koller, R., and Anderson, D., "Intravenous thrombolytic therapy for acute ischemic stroke; Weighing the risks and benefits of tissue plasminogen activator", Postgraduate Medicine, April 1998.
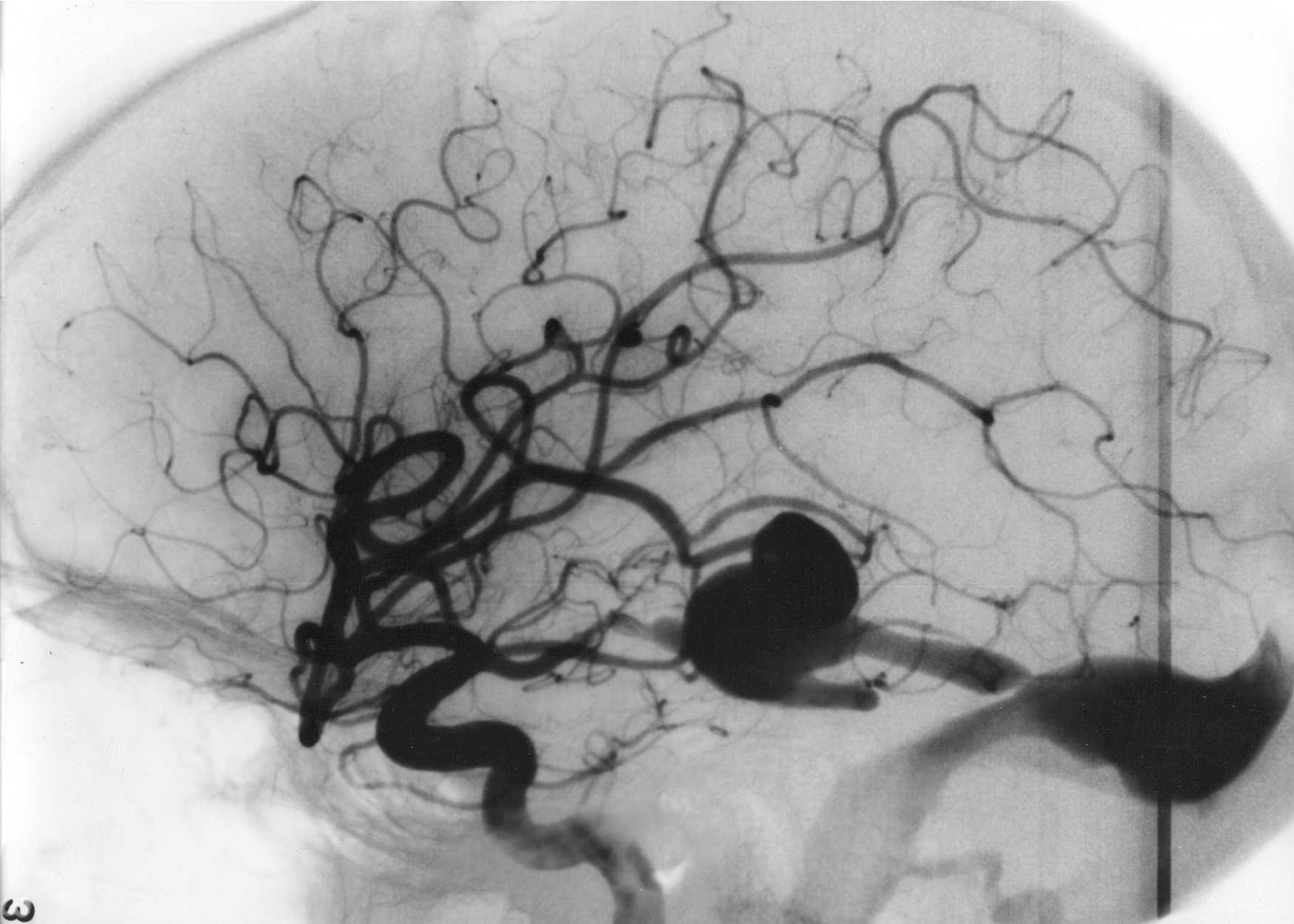
6. Wong, B., "Cerebral berry aneurysms: Diagnosis and treatment", Applied Radiology, March 1997.
7. Bard, J., "Imaging for acute stroke: Newer, faster techniques to help guide therapy", Applied Radiology, September 1997.
8. Tortorici, M.,Advanced Radiographic and Angiographic Procedures, F.A.Davis, 1995.
9. Woodward, P., and Freimark, R., MRI for Technologists, McGraw-Hill, Inc., 1995.
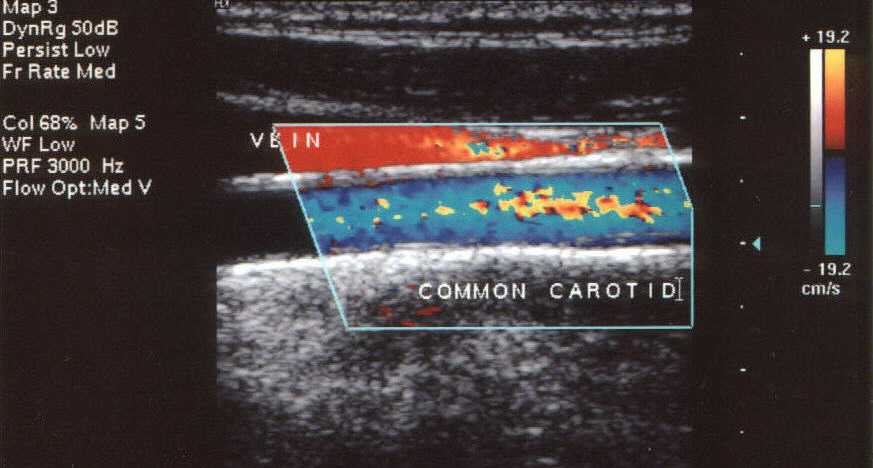
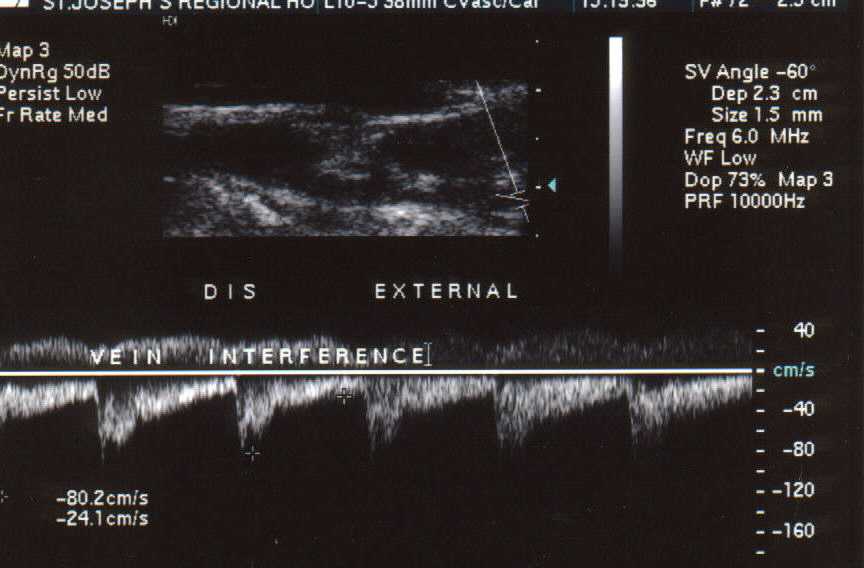
10. Nayak, S., "Noninvasive imaging of the carotid bifurcation", Applied Radiology, March 1997.
11. Taveras, J., and Ferucci, J., Radiology: Diagnosis-Imaging-Intervention, Vol. 3, Chapter 42, Debrun, G., and Breiter, S., "Arteriovenous Malformations", Lippincott, 1994.
12. Sanders, R., Clinical Sonography, A Practical Guide, Little, Brown, and Company, 1991.
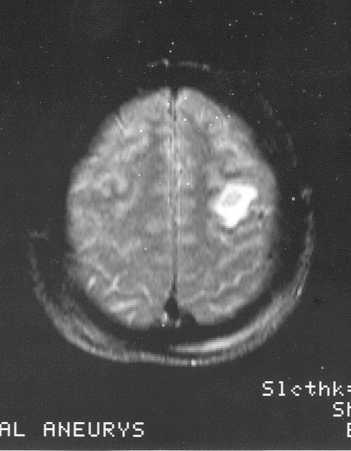
13. Dunithan, A., Cox, L., and Long, B., "Detection of Acute Stroke With Diffusion Weighted Imaging", Radiologic Tecchnology, Vol. 69, No. 6, July/August 1998.
14. Hickman, Michael, M.D., Personal conversation at National Park Medical Center, Hot Springs, Arkansas, November 16, 1999.
15. Taveras, J., and Ferucci, J., Radiology: Diagnosis-Imaging-Intervention, Vol. 3, Chapter 32A, Edelman, R., Vezina, L., and Crawley, A., "Magnetic Resonance Angiography: Special Reference to the Nervous System". |