![]() Aortic Arch and Branches
Aortic Arch and Branches
![]() Anterior Cerebral Circulation
Anterior Cerebral Circulation
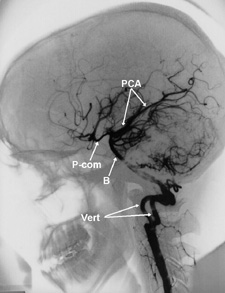
![]() Posterior Cerebral Circulation
Posterior Cerebral Circulation
![]() The Circle of Willis
The Circle of Willis
|
Medical imaging of Cerebrovascular Disease Unit 2: Anatomy of the Cerebrovascular System This unit includes a review of arterial anatomy relevant to our discussion of cerebrovascular disease. You may access an enlarged version of the radiographic images where indicated for better viewing. Click on the links below to view each topic area. This page has several images, so please be patient as they are downloaded. |
|
|
|
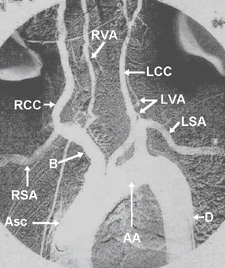
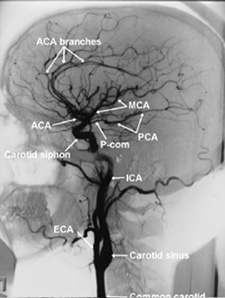
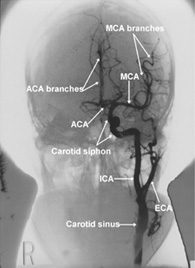
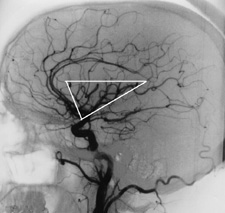
The aorta (Fig. 2.1) arises from the left ventricle and is divided into 3 segments, the ascending aorta (Asc), aortic arch (AA), and descending aorta (D). The path of cerebral circulation begins with the three major branches of the aortic arch. These are, from proximal to distal, the brachiocephalic, or innominate artery (B), the left common carotid artery (LCC), and the left subclavian artery (LSA). The brachiocephalic extends posteriorly and toward the right for approximately 5 cm. (2 inches) until it gives off the right common carotid artery (RCC) superiorly and continues laterally as the right subclavian artery (RSA). Adjacent to the RCC, the right vertebral artery (RVA) has its origin from the right subclavian. The left subclavian artery (LSA) extends superiorly from the arch and curves laterally toward the left. The left vertebral artery (LVA) has its origin from the left subclavian.4 The right and left common carotid arteries bifurcate into the external carotid and internal carotid arteries at about the level of the fourth cervical vertebra (C4). The external carotid arteries and their branches supply the neck, facial structures, and scalp. Branches of the external carotid include the facial, lingual, and superior thyroid arteries anteriorly, and the ascending pharyngeal, occipital, posterior auricular, superficial temporal, and internal maxillary arteries posteriorly.1 Cerebral circulation is directly supplied by four arteries, the right and left internal carotid arteries, and the right and left vertebral arteries (Fig. 2.2, 2.3). The first segment of each internal carotid artery (ICA) is a slightly dilated area called the carotid sinus, which performs an important function in the regulation of blood pressure. The carotid sinus contains pressure receptors within its walls which, when stimulated, initiate vasodilation, a decrease in heart rate, and a drop in blood pressure. During an angiographic procedure, carotid sinus massage may be performed to stimulate this response if the patient's blood pressure becomes elevated, but should always be done with caution and never on both sides simultaneously. Each ICA enters the cranium through the carotid canal at the base of the skull. It takes an S-shaped course beside the sella turcica, an area referred to as the carotid siphon, and ends in bifurcation laterally and posteriorly to the anterior clinoid process.1 The branches of the ICA supply the anterior, middle and lateral portions of each cerebral hemisphere. The major cerebral branches of the internal carotid artery are the anterior cerebral and middle cerebral arteries, and the posterior communicating (P-com) artery which joins the ICA to the posterior cerebral artery, forming a segment of the Circle of Willis. Notice the cross-filling of contrast from the anterior circulation across the P-com into the PCA in Fig. 2.2 Each anterior cerebral artery (ACA) courses medially to form the anterior segments of the Circle of Willis (Fig. 2.3, 2.6), then courses superiorly, branching to supply the frontal lobe, basal ganglia, and portions of the parietal, and temporal lobes including the lateral ventricles and corpus callosum.2 The right and left ACA's are joined across the midline by the short anterior communicating (A-com) artery to complete the anterior portion of the Circle of Willis. Notice in Fig. 2.3 the cross-filling of contrast from the left ACA across the midline via the A-com into the right ACA circulation. Radiographically, the branches of the ACA delineate the midline as they outline the medial surfaces of the frontal and parietal lobes, within the longitudinal fissure. Displacement of these vessels from their normal position as seen on a frontal angiographic image is referred to as "midline shift", and indicates the presence of a nearby mass, such as an aneurysm, edema, hematoma, or tumor. As the mass encroaches upon and displaces healthy tissue, injury can result. This is referred to as the "mass effect". Embolism involving the anterior cerebral is relatively uncommon.3 The middle cerebral artery (MCA) is the largest branch of the internal carotid artery, and serves large portions of the frontal, parietal, and temporal lobes, including the basal ganglia, motor, sensory and auditory areas, and the lateral surface of each cerebral hemisphere.1, 2 It extends horizontally and laterally from its origin before branching at the Sylvian fissure. The subsequent ascending branches outline the insula, a triangular shaped area of the cerebrum at the floor of the Sylvian fissure. The appearance of these vessels in this area, referred to as the Sylvian triangle, is diagnostically important, and can be best observed on the lateral projection of an internal carotid arteriogram. The MCA is the most commonly affected vessel in embolic stroke.3 |
Fig. 2.1 Click to enlarge. The aortic arch and its branches.
Fig. 2.2 Click to enlarge. Normal branches of the left internal carotid artery, lateral view.
Fig. 2.3 Click to enlarge. Normal branches of the left internal carotid artery, frontal view.
Fig. 2.4 Click to enlarge. The Sylvian triangle, formed by branches of the middle cerebral artery. The inferior point of the triangle denotes the origin of the MCA. The superior horizontal margin outlines the superior aspect of each of the insular loops of the MCA branches. Displacement of these structures can indicate a mass effect, while absence of some or all of the branches will indicate embolus or thrombosis. |
|
Fig. 2.5 Click to enlarge. Normal circulation of the vertebral arteries and branches.
Fig. 2.6. Inferior view of the Circle of Willis. |
Posterior Cerebral Circulation As previously mentioned, the right and left vertebral arteries have their origins from the right and left subclavian arteries respectively. The vertebral arteries (Fig. 2.5) course superiorly on either side of the cervical vertebrae, passing through each of the transverse foramina from C6 through C1. They enter the cranium through the foramen magnum, and join to form the basilar artery. The basilar artery (B) extends superiorly and anteriorly from the area just in front of the medulla oblongata, past the pons and along the surface of the clivus. The basilar artery bifurcates into the right and left posterior cerebral arteries (PCA). Each PCA supplies the occipital lobe, medial and lateral occipitotemporal surfaces, third ventricle, posterior basal ganglia and midbrain structures.1 Each PCA also joins with the respective posterior communicating artery (P-com), forming the posterior segments of the Circle of Willis. Notice in figure 2.5 the cross-filling of contrast via the P-com into portions of the anterior circulation. Because the two vertebral arteries join before continuing into the posterior circulation, catheterization of both during arteriography is not usually necessary. Because the LVA is usually slightly larger in calibre than the right and arises at a less acute angle from its origin, it is usually selected for catheterization. The contrast will often reflux into the opposite vertebral artery during injection, thereby demonstrating both vessels with a single contrast injection. Notice the bilateral filling of both vertebral arteries demonstrated in Fig. 2.5. The Circle of Willis The Circle of Willis is a central junction of vessels at the base of the brain which joins the anterior and posterior cerebral circulations (Fig. 2.6). The Circle provides an important route of secondary, or collateral, circulation in the event of loss of circulation from one of the vessels, and is the most common intracranial collateral pathway.1 Although variations exist among the population, its general structure is that of each distal internal carotid artery (ICA) connected to an anterior and posterior segment. The anterior segment includes the right and left anterior cerebral arteries (ACA) joined by the very short anterior communicating artery (A-com), while the posterior segment includes right and left posterior communicating arteries (P-com) joined to respective posterior cerebral arteries (PCA). Figure 2.6 represents an inferior view of the base of the brain, with the vertebral (RVA,LVA) and basilar (B) arteries indicating posterior circulation. The Circle of Willis is the most common location for congenital "berry" aneurysms. Aneurysms of the anterior communicating artery constitute 34% of all intracranial aneurysms, while those of the first segment of the anterior cerebral artery account for 28%.4 |
References
|
1. Uflacker, R., Atlas of Vascular Anatomy, An Angiographic Approach, Williams & Wilkins, 1998. |
|
ÜBACK |
NEXTÞ |
Back to Home | Review Questions | Glossary | Go to Test | Go to Survey
Ó
Images and text copyright Ken McCormick, April 1999. All rights reserved.