Approaches to Interpretation of Plain Radiographs
![]()
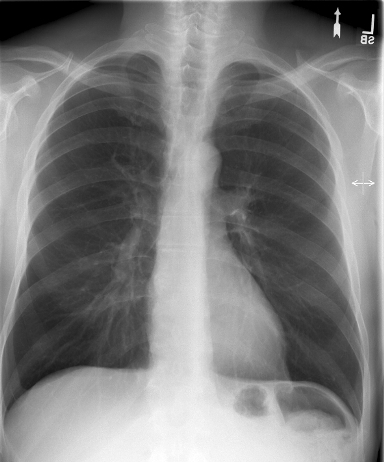
Chest
PA
| Who, What, Why? | |
| Prior imaging | oldest & most recent |
| Technical quality | Rotation (spinous processes equidistant from medial end of clavicles)
Inspiration (6 - 7 anterior ribs in MCL) Penetration (spinous processes visible) |
| Lines, tubes | ETT: 5 cm sup to carina [just sup to arch] [has excursion +/- 2 cm] Trachoeostomy tube tip: 1/2 to 2/3 from stoma to carina CVC: SVC (if RA → may arryth or perforatn) S-G: < 2 cm lat to hila NGT: > 10 cm w/n stomach FT: lig of Trietz
Neonate: |
| Abdomen | Diaphragm, pneumoperitoneum, colonic interposition, costophrenic angles, subpulmonic effusion (highest point of hemidiaphragm displaced laterally), tension pneumothorax |
| Thoracic cage | #'s, lesions, notching, pneumothorax |
| Mediatinum | Heart (size, contour), great vessels, airways, esophagus, LN's, AP window, paratracheal stripe, paraspinal lines, ant & post junction lines, azygoesoph recess |
| Lung parenchyma | CPA, apices, volumes, vascular markings, lesions (including behind heart & diaphragm), pneumothorax |
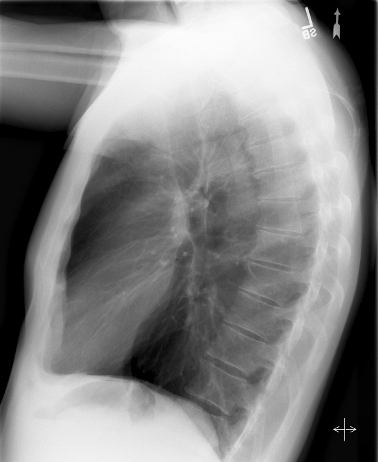
Lateral: diaphragm, CPA, spine sign, hilar LAD, posterior wall of bronchus intermedius, upper lobe bronchi, retrosternal space
-
Opacity
Etiologies: Blood, pus, fluid, cells, protein
Common findings in ICU: edema, atelectasis, effusion, cardiomegaly, life supports
Cardiogenic pulmonary edema progession:
� vascular redistribution
� interstitial pulmonary edema (perihilar haze, peribronch cuffing, Kerley A & B lines)
� alveolar pulmonary edema
� pleural effusion
| Air-space disease | Fluffy margins
Acinar shadows (7 mm) Air bronchograms Silhouette sign Homogeneous (when acinar consolidation confluent) Non-segmental distribution (d.t. intersegmental channels) |
| Interstitial disease | Ground-glass (granular)
Reticular (fine, medium, coarse; Kerley A, B, C lines; acute: hazy, not distorted; chronic: sharp, distorted) Nodular Reticulonodular Honeycomb (5 - 10 mm) |
| Atelectasis | Volume loss, no air bronchograms if resorption atelectasis
Resorption (e.g. d.t. mucus plug) Relaxation (passive) Adhesive (e.g. d.t. abnl surfactant) Cicatrization (d.t. pulmonary fibrosis) |
| Benign Nodule | Size: <2 cm
Margins: well-defined, smooth Calcification: laminated, multiple punctate, or popcorn Fat indicates hamartoma Growth: none over 2 yrs Age: below 40 y/o |
Pleural Effusion
Can see 25 mL on lat decub
Can see 300 mL on PA
Mediastinal Masses
| Anterior | Thyroid
Thymoma Teratoma Terrible lymphoma |
| Middle | Lymphadenopathy
Esophageal mass Hernia, Hematoma Aneurym Bronchogenic cyst Inflammation (sacoidosis, T.B., histoplasmosis, coccidioidomycosis) Tumor |
| Posterior | Aneurysm
Neurogenic tumor Spine mass |
Aortic Disruption
left Bronchus depressed
left pleural Effusion
widened Mediastinum
apical Cap
Aortic knob indistinct
Trachea deviated to right
Asbestos-related pleural disease: pleural plaques, diffuse pleural thickening, pleural calcification, benign effusion
Pleural calcification without h/o surgery, TB, empyema, hemothorax, etc. is pathognomonic of asbestos exposure.
Asbestosis is asbestos-related interstitial pulmonary fibrosis
![]()
Abdomen
| Prior imaging | oldest & most recent |
| Lines, tubes | E.g. NGT, Dubhoff feeding tube |
| Stones | Nephrolithiasis, cholelithiasis |
| Bones | Ilioishial line, iliopectineal line, arcuate lines, Shenton's arc, coxa vara or valgus, protrusio acetabuli, anterior & posterior rim lines, femoral head, bone texture, joints |
| Mass | |
| Gas | Obstruction, ileus |
![]()
Musculoskeletal
Stability = Propensity to further displacement
Fractures
| Prior imaging | oldest & most recent |
| Location | E.g. proximal, middle, distal third |
| Type | E.g. transverse, oblique, spiral, comminuted, green stick, torus, stress, insufficiency |
| Joint involvement | |
| Displacement | E.g. 50% posterior |
| Angulation | E.g. vertex medial |
| Rotation | |
| Over-riding / distraction | |
| Effusions | |
| Soft tissue swelling | |
| Hardware | Correct positioning, lucencies, osteomyelitis, #'s
E.g. intramedullary rod, dynamic hip screw, spinal fusion plate & screws, k-wires, cortical screws, cancellous screws,cerclage wire, tension band wire, external fixator Orthopedic hardware |
![]()
Tooth Numbering System
![]()
C-Spine
| Prior imaging | oldest & most recent |
| Bodies | Height, trabeculations |
| Disks | Height, |
| Odontoid | #'s, dens-anterior arch distance (adults: < 3 mm; peds: < 5 mm) |
| Lines | Anterior spinal line, posterior spinal line, spinolaminar line, clivus base line |
| Lordosis | |
| Soft tissue swelling | Retropharyngeal, retroesophageal |
L-Spine
Degenerative Disease of Spine
| Degenerative disk disease (DDD) | ↓ disk space osteophytes borders of adjac vert bodies may vacuum phen |
| DISH | flowing ossifn >= 4 contig verts no facet or SIJ ankylosis rel minimal DDD |
| Spondylosis deformans | ant & lat osteophytes rel preserved disk spaces |
| Facet DJD | osseous facet overgrowth ↓ jt space sclerosis |
Facet DJD + DDD may → degen spondylolisthesis
Scheuermann's disease
- Categorized as an "osteochondrosis"
Possibly a growth disorder of vertebral bodies (poorly understood)
Typically 13-17 y/o with back pain
Lower thoracic spine involved most frequently
- Radiographs:
Multiple Schmorl's nodes
Disk space narrowing
Endplate irregularities
Anterior wedging
Changes seen in >3 vertebral bodies (with > 5 degrees anterior wedging in each)
Kyphosis usually > 35 degrees

![]()
Shoulder
| A-C joint | 3 - 8 mm |
| Coracoid - clavicular distance | 10 - 13 mm |
| Glenoid - humeral distance | ?8 mm |
![]()
Acetabulum
Ileopectineal Iileopubic) line
Ileoischial line
Tear drop
Posterior rim
Superior rim
Anterior rim
![]()
Ankle Fracture
Medial malleolus
Lateral malleolus
Posterior malleolus
Base of 5th metatarsal
Dome of talus
Lateral talar process
Anterior calcaneal process
Lateral calcaneal process
Proximal fibula
Soft tissue swelling
![]()
Arthritides
| Osteoarthritis
"Wear & tear exceeds repair." | Subchondral sclerosis
Osteophytes Asymmetric joint space narrowing Pseudocysts |
| Rheumatoid arthritis | Erosions
Symmetric joint space narrowing Soft tissue swelling Osteopenia (periarticular) |
| Charcot joint | Joint destruction
Heterotopic bone formation Subluxations |
![]()
Bone Tumors
Margins
| I - Geographic | A - well-defined & sclerotic B - well-defined & not sclerotic C - ill-defined | usually benign usually benign not ... |
| II - Moth-eaten | ||
| III - Permeated | ||
Periosteal Reaction
Aggressive: sunburst, hair-on-end, Codman triangles, laminated
![]()
Osteomyelitis
Plain films (require 10-14 days to develop):
-
STS
Periosteal reaction
Lytic changes (Require 2-6 weeks and reflect 50-70% bone density loss. Antibiotic use may arrest bone mineral loss.)
-
Can diagnose osteomyelitis within 3 days of symptom onset. 95% sensitive and specific.
False positives: healing fractures, prostheses, neuropathic osteoarthropathy.
In this instance, Indium-labeled WBC images are superimposed on the bone scan.
Approaches to Interpretation of Plain Radiographs
Approaches to Interpretation of CT
Approaches to Interpretation of MRI
Sample Normal Dictations
Sample Chest Dictations
Sample Nuclear Medicine Dictations
Normal Values
Chest Differentials
GI Differentials
Nuclear Medicine Gamuts
Chest Radiology Gamuts
Links
Multinodular Disease: A High-Resolution CT Scan Diagnostic Algorithm