
|
|
|
An
Aneurysm
is a dilatation, stretching, and bulging of an a artery that occurs as a
weakening of the arterial wall and loss of usual elastic properties. Aneurysm
is derived from the Greek word " aneurysma" meaning "a widening". They can
occur in any artery in the body but are most common in the aorta- the main
artery of the body that carries blood from the heart to the rest of the body.
Abdominal Aortic Aneurysms (AAA) are seen in the abdominal segement of the aorta and are most common after age 60; they are 5
times more common in men than women. Approximately 5% of men over age 60
develop AAA.
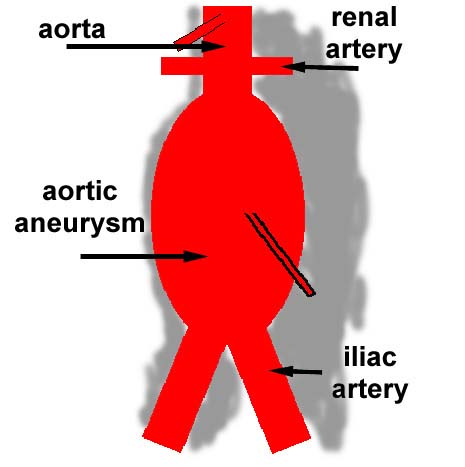
90% of aneurysms occur below the level of the renal arteries, and can involve
the bifurcation of the aorta into iliac vessels ( arteries supplying the legs).
They are fusiform, i.e. like a spindle with widening all around the
circumference.
What are the causes of AAA?
80 % of AAA are caused by
atherosclerosis
which can weaken the aortic wall, then the pressure of the blood pumped in the
aorta causes expansion at the weak site.
Other causes include:
The fact that large aneurysms can remain undetected, until they suddenly
rupture is what makes them so potentially dangerous.
What do AAA look like?
How are AAA found?
Most of the time it is an incidental finding during a routine medical visit, or
most commonly when a test
ultrasound
or
CT Scanner/MRI Scanner
is done for other completely separate reasons( kidney, gallbladder, prostate ).
Very occasionally, a patient may discover the AAA by becoming aware of an
abnormal pulsating mass in the center of his/her abdomen.
Because AAA often remain symptomless and undetected for years, some of them,
unfortunately are diagnosed when they rupture. This is why all living (> 50 years of age) siblings
of a patient with ruptured AAA, should get an abdominal ultrasound to make sure
they do not have one.
Do all AAA need repair?
The need for intervention depends on the symptoms, the size of the AAA, and the
general condition of the patient.
The normal size of the adult male aorta is 2 - 2.5 cm, moderate dilatation up
to 4 cms is seen in 4 % of males over the age of 65 years.
Small aneurysms ( smaller than 5.5 cm) do not require repair unless they become symptomatic, they are however kept under careful surveillance with repeat ultrasound scans to ensure that they do not enlarge.
Larger aneurysms ( 5.5cm and above) carry an increased risk of sudden rupture. Most vascular surgeons would consider elective surgical repair if the patient's general medical condition allows it.
 .
.
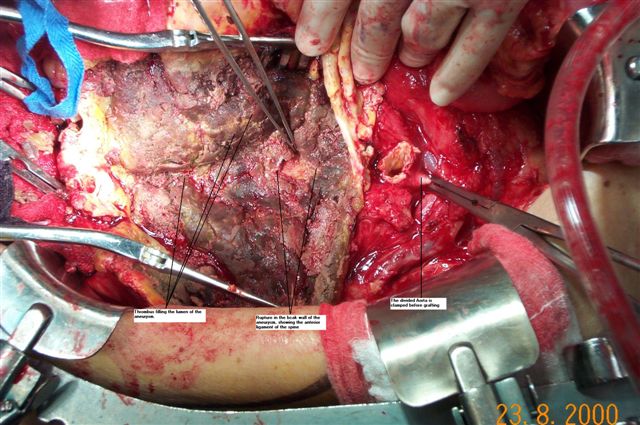
This is a major surgical procedure done under general anesthesia, invasive
monitoring, and through an abdominal incision during which the abdomen is
opened, the aorta is then temporarily clamped. It is usually possible to apply
the clamp below the renal arteries, thus allowing continuous flow to the
kidneys during the repair. Blood flow to the legs is interrupted, but is not
usually a problem for the duration of the surgery ( +/- 2 hours ).
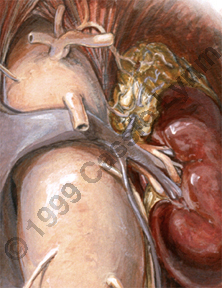
AAA contain blood clot and debris, that are removed, then the graft is sawed
to the normal caliber aorta above and below the opened AAA so that it lies
wihtin what was the inside of the aneurysm. Some aneurysms need to be repaired
by extending the lower end to the femoral arteries in the groin. At the end of
the procedure, the wall of the AAA is wrapped around the graft to isolate it
from the bowel and other surrounding viscera.
Most patients will be monitored in an Intensive Care Unit ( ICU) for the first 48 hours and will be discharged from the Hospital after 7 days. Full recovery, however will take 6 - 8 weeks.
Over the last few years, less invasive methods have beed researched to avoid a
major open repair, the new procedure is called " EndoVascular Aneurysm Repair" or EVAR. It
involves passing a graft into the inside of the AAA through the femoral artery
in the groin. Careful x-ray measurements are taken before, during and after the
procedure.
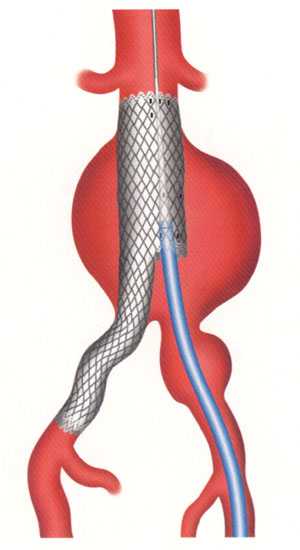 The graft is fixed in place using a specially devised metal "stents" attached
to the graft. Repeat CT Scanners are required in follow up to monitor the
position of the graft and other important and relevant findings.
The graft is fixed in place using a specially devised metal "stents" attached
to the graft. Repeat CT Scanners are required in follow up to monitor the
position of the graft and other important and relevant findings.
This technique is still being refined, multiple studies and protocols all over the globe are being carried out to deal with the safety and long lasting blood-tight seal at the end of the graft. It seems unlikely that endovascular techniques will ever be suitable for the repair of all shapes and sizes of aneurysms but do offer a minimally invasive surgical option and shorter hospital stay. It is becoming safer and offered in Canada more freely and at more centers.
Repiratory complications can occur after any abdominal surgery, by limiting the ability of deep breathing and coughing. Epidural anesthesia and intensive post-operative chest physiotherapy can minimise this risk.
Bleeding is an obvious risk in an operation on the major artery of the heart, especially that blood thinner( Heparin) is used when the aorta is clamped to prevent blood from clotting. Blood loss during AAA repair averages 500 to 1000 mls or cc , most patients require blood transfusion during or after the operation. You can donate your own blood in the 2 to 3 weeks preceeding your surgery if you are concerned about blood transmitted disases/reactions.
Heart is the single greatest source of post-operative complications/mortality. Most patients are older than 60, are smokers, and have associated underlying heart conditions. Normally the patient is seen by a cardiologist to correct and control the underlying heart disease, some patients will see their surgery cancelled because of poor heart condition, rendering surgery very risky.
"Blocked graft" can occur when the repair involves the iliac/femoral arteries. It is rare and can occur either within the first 24 hours or few years down the road. It will require another operation.
Sexual function can be damaged in men in the form of poor/absent erection or failure to ejaculate. The former occurs when the blood vessel supplying the penile muscles are involved in the aneurysm or its repair, the latter occurs when the nerve fibers are damaged.
It is important to mention that patients who have undergone successful aneurysm repair have an average life expectancy almost identical to that of normal popualtion of the same age.
Ruptured AAA
This is a complication that should be avoided because of its high morbidity and
mortality. It occurs when the dilated, stretched wall of the aorta begins to
tear under the pressure of the blood within it. Blood escapes either into the
tissues surrounding the aorta in the back of the abdomen, or freely into the
abdomen.
The rupture may cause sudden, rapidly fatal blood loss, or may cause smaller bleeds, associated with abdominal , back or groin pain, progressing over a matter of hours or days to massive life threatening bleeding. Without proper treatment, a leaking aneurysm leads inevitably to death. Most of the time the patient will experience low abdominal or low back pain, or loss of consciousness.
Rupture of AAA is responsible for an estimated 25,000 deaths annually in the US, it remains the 13th leading cause of death. It is estimated that less than half of all patients with ruptured AAA will reach hospital alive and, of those less than half will survive emergency surgery. Complications following successful repair are many times more common than elective repair.
{kind=link}
{kind=link}
{kind=link}