|
|
|
Basically it means a clot in the vein. As the venous system is divided in deep veins and superficial veins one can have clot in each of the systems. Only very rarely clotting can occur in both of the systems in the same time.
Superficial vein thrombosis is also called superficial thrombophlebitis/phlebitis. The "itis" denotes that the vein is engulfed in an inflamatory process: the skin around the vein is red and painful. Swelling can be present as well. Unfortunately, many physicians treat this condition with antibiotics. This is completely unnecessary as in most of cases there is no bacterial infection.
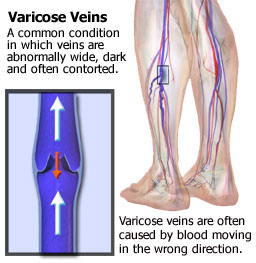
The main cause for the condition are varicose veins. Blood stagnates in those venous pools and will clot easily especially during inactivity. Injecting varicose veins can lead to superficial phlebitis as well. In the absence of varicose veins one should look for other reasons such as malignancy elsewhere in the body, gout, Buerger's disease. or an inherited tendency to clot.
The treatment of the condition is simple: evacuation of clot if the patient comes early to the physician, local compression with ace bandages or surgical stockings, and ambulation. The only medication to be given is ibuprofen (Motrin/Advil) or Aspirin 5-7 days that will ease the pain and calm the inflamatory reaction.
Occasionally Superficial Phlebitits can be associated with DVT. Only in these cases is anticoagulation treatment necessary. If the underling condition for the superficial phlebitis was varicose veins after the inflamatory process has cooled off, surgery for the varicose veins is indicated.
Deep vein thrombosis (abbreviated as DVT) is ussually localized in the deep veins of the calf but it can extend into the deep veins of the thigh and even beyond. The more extensive the clot the more dangerous the condition is. Among the clinical signs are calf pain and swelling (edema) of the ankle and possibly calf. It is potentially a dangerous conditions as a piece of the clot can "fly" through the venous circulation and lodge in the lungs occluding the pulmonary circulation. This is called pulmonary emboli or PE. It can be fatal if it is massive.
Damage to the deep vein valves by the retracting clot in the ensuing months could leed in a few years to venous circulatory problems in the leg that if not treated with compression can evolve even into skin ulceration. This is chronic venous insufficiency and venous ulceration repectivly.
The main question the physician has to find out why did DVT occur in the first place? There is always a 25% DVT risk even in healthy people who undergo surgery under general anesthesia. After 40 years of age, and/or in surgery fo cancer, hip, urological procedures , brain and gynecological surgery the incidence of post operative DVT is even higher. Prevention is the best treatment. One should always ask the surgeon and the anesthetist what are the methods they will use to prevent DVT to occur during surgery. Usually they are mechanical (compressive devices) and pharmacological (low dose of subcutaneous injections of Heparin or any of the soon to become available anticoagulant pills).Long distance travel by car or by airplane can induce DVT as well just by calf inactivity. In debilitating diseases with lengthy bed rest the mechanism is identical: calf pump inactivity and blood stagnation. Cancer in a distant organ can manifest itself with a calf DVT! Once with DVT a person is prone to develop another one. If it is a recurring condition without obvious reason, the blood should be checked ( blood tests) to rule out rare congenital hypercoagulability states such as seen in defficiency in protein S or C, antithrombin III, or presence of lupus anticoagulant.