| ENS tutorial (3) |
 |
| OK, so if the airflow is an issue, then what can be done about this? My idea is to implant the nose with tissue to both limit the airflow overall, and to redirect the flow to attempt to approximate a pre-surgical state. The normal state can likely never be achieved, but we can try our best. Materials such a Alloderm (TM), etc. can be placed within the nose - preferably below perichondrium or preiosteum, to form a pseudo-turbinate. People often ask me why a new inferior turbinate cannot be manufactured. The problem is the size of the tissue, its complexity, and its blood supply. The inferior turbinate is the size of your index finger. It has bone, submocosal capacitance vessels, and overlying mucosa. The majority of its blood supply comes in posteriorly (below the sphenopalatine foramen), enters the bone, and fans out into the turbinate as it proceeds anteriorly [simplified explanation]. Anastomosing that blood supply is not possible with todays technology, even if we could "grow" a complex structure such as a turbinate in a petri dish, which we cannot. We can grow cartilage relatively well, mucosa can be grown somewhat. Yes, advances will be made in these avenues, but they are still a long ways off. |
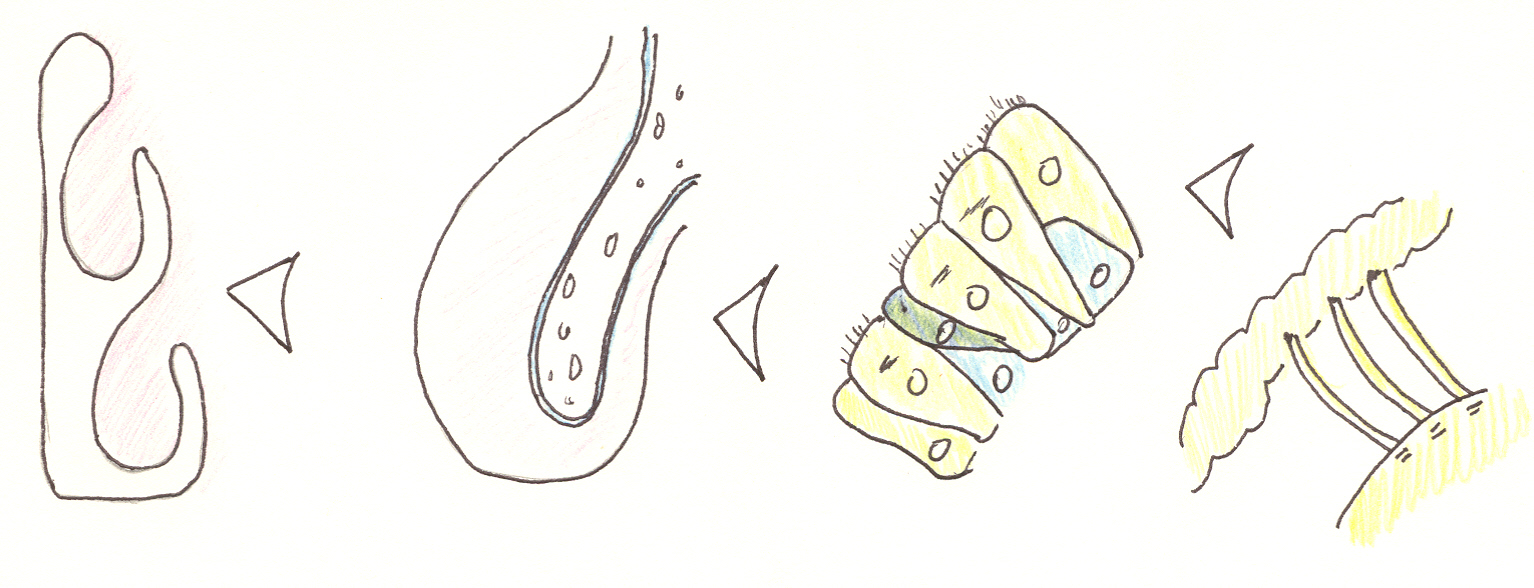
| Progressive "blow up" of normal nasal anatomy showing a left coronal view, the left inferior turbinate with periosteal covered bone, normal nasal mucosa (pseudostratified ciliated columnar), and nasal cilia interacting with the gel and sol layers of the nasal mucus. |
 |
 |
 |
| 1) depicts a patient with ENS-IT who has had tissue implanted. The airflow is indicated with colors again. Obviously this looks great in a drawing, but achieving these results practically is not as easy. 2) shows a patient with ENS-MT with an implant in position. 3) shows a patient with ENS-both with a large implant in position. Obviously these are 2 dimensional pictures, trying to represent a 3 dimensional implant. The location of the implant is quite important. |
| What about sensation issues? I do feel that sensation may possibly be damaged/impacted from surgery. This may explain why some subjects describe ENS symptoms, yet their anatomy is, for all intensive purposes, fine. As we really do not have a great explanation for ENS even with anatomical changes, this situation gets even harder to define. If we had a good way to assess the nasal sensation to airflow, we might be able to better define this. My project to measure the sensation to nasal airflow has had IRB approval, but I have never secured the funding to proceed. I'd love to have more answers to this dilemna. |