 |
| ENS tutorial (2) |
 |
| Note that most of this information is my opinion after evaluating a large number of ENS (empty nose syndrome) patients. Little of this information is within any textbook. My thought are based upon observations, not upon studies. These theories are simply that - works in progress. Please do not accept everything I have written here as proven true. I am including this information for those who wish to share more in depth analysis of the ENS condition. The picture to the left depicts a coronal section of a normal left nasal cavity. The septum, middle, and inferior turbinates are intact. The "speed of airflow" is suggested by the color: red is very fast, while orange and yellow are slower. The nasal airflow is laminar in normal circumstances, but it hovers upon being turbulent. In fact a sniff drives the flow into a turbulent state and allows more air to enter the olfactory region in the most superior aspect of the nasal cavity. |
Rapid airflow dries the mucus layer - dessicated crusts further limit the ability for airflow to strike the mucosa to trigger sensation. I am of the opinion that the sensation to flow is a combination of information from the nares (nasal vestibule) and the region of the middle meatus. |
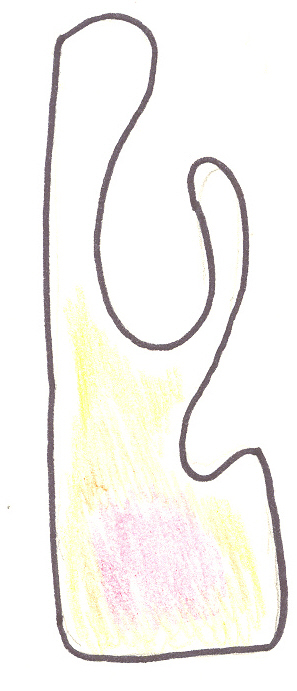
| Now in this coronal section, a person has had their inferior turbinate resected. As the color indicates we have rapid airflow along the floor of the nose (away from the middle turbinate region). Can this person breathe? Absolutely - they can entrain a huge amount of air. Can they tell that they are breathing? This is where ENS becomes more difficult. Most patients with the anatomy in the picture do NOT complain of any breathing difficulty, while others (yes, a minority of patients) feel they are suffocating. Why the difference? Why would most patients not note any difficulties, while some are MISERABLE after such a procedure? I cannot answer why exactly, but I suspect it is (1) a function of airflow differences between these individuals, and (2) differences in mucosal sensation. |
| Can this problem occur with the middle turbinate being resected? It appears that this can occur, though the smaller size of the middle turbinate, and therefore its smaller alteration of the overall airflow patterns, makes it less common. The airflow in this case is toward the middle meatus region as well, which may make the sensation of paradoxical congestion less of a factor. Pain may become more of an issue though, as the airflow is coursing toward the area where the sphenopalatine nerve exits from its bony canal in the sidewall of the nasal cavity. This site is indicated with the pointer; it lies posterior to the normal maxillary antrostomy. |
 |