|
Herpes
Simplex Virus
There are two closely related viruses termed :
herpes simplex virus type 1 (HSV1), and
herpes simplex virus type 2 (HSV2).
Both
viruses cause painful vesicles on the skin at
the site of inoculation.
HSV1
is usually associated with oro-facial lesions.
HSV2 is usually associated with genital lesions.
EPIDEMIOLOGY
Infection with HSV1 is almost universal. This
is known because, although many infections are
sub-clinical, virtually 100% of adults have antibodies
in their serum. Most individuals become infected
in the first few years of life.
Virus is shed from the infected area and spread
occurs as a result of direct contact with lesions.
For example, through kissing (HSV1) or sexual
intercourse (HSV2).
Virus may also, however, be shed in saliva and
genital secretions and can thus be transmitted
in the absence of clinical lesions.
CLINICAL FEATURES
There are 2 clinical patterns of disease:
a)
Primary Infection , and
b)
Recurrent disease
Primary
Infection
Most primary infections are silent.
In clinically apparent cases, vesicles usually
develop at between 1-3 days post exposure and
remain localized to the site of inoculation. However,
in immunocompromised individuals the virus may
disseminate.
The
nature of the disease is determined by the site
of inoculation:
Gingivo-stomatitis
This is the most common form of primary infection;
inoculation is usually through kissing. There
is a wide spectrum of severity, from trivial to
extensive disease. Painful vesicles develop inside
the mouth on the bucchal mucosa and gums, on the
lips and skin around the mouth. The vesicles inside
the mouth ulcerate and become covered with a greyish
slough. Lesions may occur at other sites on the
head and neck as well.
The primary eruption is often associated with
fever and cervical lymphadenopathy. The illness
is self limiting and lesions usually heal within
14 days.
Kaposi’s
Varicelliform eruption
Super-infection of eczematous skin with HSV.
Herpetic Whitlow
Inoculation of virus into the fingers - an occupational
hazard of doctors, nurses and dentists.
May be mistaken for a paronychia and incised .
Conjunctivitis,
Keratitis
Herpetic
lesion on the cornea - is called a dendritic ulcer
because of its branching appearance. Pain and
photophobia are prominant features. Conjunctivitis
and oedema of the lids commonly accompany primary
infection. Lesions usually heal within 3 weeks.
Genital
Herpes
Sexually transmitted herpetic lesions. Usually
due to HSV2 but 20-30% of cases are due to type
HSV1. Primary eruption lasts ±10-14 days.
Acute necrotizing encephalitis
Infection of the brain by HSV. Neurons of the
temporal lobe are most commonly involved. Infection
is severe and necrotising. Clinical features include:
sudden onset of fever, headache, confusion and
alteration in personality. Mortality is high and
neurological impairment in the survivors is invariable.
Encephalitis may be due to primary infection or
reactivation.
Neonatal Infection
This is a very rare condition. Neonates have poor
cell mediated immunity and are therefore at increased
risk of disseminated infection if they are exposd
to HSV in the perinatal period.
Exposure
may occur:
1) at birth, if the mother has genital herpes
at the time of delivery. (This is only a significant
risk if the mother is experiencing a primary infection).
2)
In the post natal period, if the infant is handled
by people with herpetic lesions.
The
disease may take one of three forms:-
Cutaneous
lesions:-
These are confined to the skin, and the prognosis
is good.
Generalized infection:-
This is a serious condition, with a high fatality
rate. Virus disseminates throughout the organs.
Cinical features include jaundice, hepatosplenomegaly,
thrombocytopenia, pneumonia and encephalitis.
Lesions on the skin may be trivial.
Encephalitis:-
Direct infection of brain tissue.
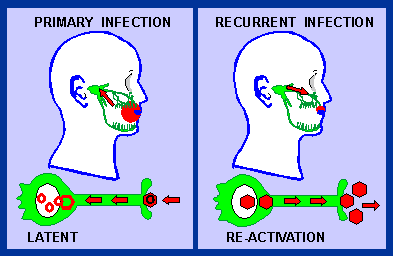
Latency
and Recurrent disease
HSV1
and HSV2 can establish a latent infection in the
ganglia of the nerves that supply the site of
the primary infection
Genital area - sacral ganglia
Oro-facial - trigeminal ganglion
Following
primary oro-facial infection, the virus enters
sensory nerve endings and travels up the axon
and establishes a latent infection in the trigeminal
ganglion.
The
viral genome persists in an episomal form (plasmid)
in the nucleus of the neurone. No viral genes
are expressed. This state of latency may persist
for many years.
In
a percentage of people,
the virus will reactivate: - A cycle of viral
replication occurs in the neurone and virus particles
travel down the axon to reinfect the skin or mucous
membrane in the area supplied by the nerve.
Reactivation
may be provoked by a number of stimuli:
including sunlight, stress, febrile illnesses,
menstruation or immunosuppression.
-
Clinical manifestations of reactivation:
1. Cold sores (follows gingivo-stomatitis):
Following one of a variety of stimuli, vesicles
erupt on the muco-cutaneous junctions of the nose
or mouth. These are more localized than the primary
infection and heal more rapidly (7-10 days). The
eruption is often preceeded by paraesthesia of
the involved area.
2.
Recurrent genital herpes:
Recurrence with HSV 2 infections is more common
than with HSV 1. Lesions are less extensive and
heal more rapidly than the primary infection.
3.
Keratitis:
The virus reaches the cornea via the ophthalmic
branch of the trigeminal nerve; the clinical lesion
is termed a dendritic ulcer. It heals more rapidly
than the primary infection.
LABORATORY
DIAGNOSIS
Direct
detection by electron microscopy of herpesvirus
particles in vesicle fluid
Culture:
Isolation from clinical material from skin lesions
may be inoculated onto cell monolayers which are
monitored for the development of characteristic
cytopathic effect. This is usually detected within
three days
Serology
is not very useful because there is a high prevalence
of antibody in the normal population.
|