Acute Tubular Necrosis
1.
What part of the nephron is affected? Why is this part most susceptible?
The
straight part of the proximal tubule and the ascending thick limb is affected
and is the most susceptible. This
is because at these regions of the nephron, a lot of active transport is carried
out, and hence a lot of oxygen is needed to replenish the ATP used in active
transport, and thus these regions are very sensitive to hypoxia.
Other factors include a vast electrically charged surface for tubular
reabsorption and the capability for effective concentration.
2.
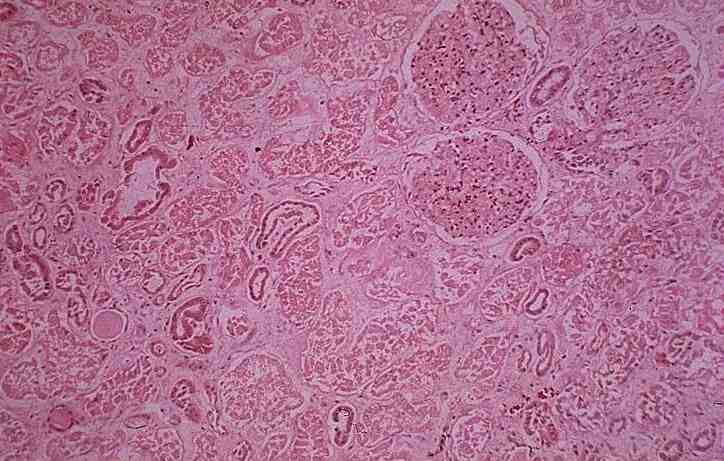
What are the histopathological features of this condition?
Anucleate, homogeneous, eosinophilic appearance on slide.
Epithelial regeneration with hyperchromatic nuclei may be seen.
Interstitial
edema.
3.
Explain the pathogenesis.
Ischemia
causes the depletion of ATP which is required for membrane transport, protein
synthesis and phospholipid turnover. Failure of Na-K-ATPase active membrane
transport causes sodium to enter the cell and potassium to diffuse out,
resulting in swelling of cell. Cell switches to anaerobic glycolysis, resulting in lactic
acidosis. The increased pH and the continued
ATP loss leads to intracellular release and activation of lysosomal enzymes. The
acidosis inhibits degradative enzymes (hence pattern of coagulative necrosis,
compare with liquefactive necrosis where degradative enzymes are active).
Eventually there is rupture of cell membrane and necrosis ensues.
Tubular function is then impaired.
4.
Name some common causes of such damage.
It
can be caused by:
1.
Ischemic damage (involving multiple portions of the nephron)
2.
Toxic damage (involving mainly the proximal tubule)
5. (a) How is renal function affected?
Reduced
GFR, leading to oligouria (decline in urine output), hyponatremia, hypokalemia,
increased blood urea nitrogen, metabolic acidosis.
(b)
List some clinical/biochemical manifestations.
Clinical:
There
are 3 phases in clinical presentation:
initiating, maintenance, recovery.
Initiating
phase (36hrs): slight decline in urine output; rise in BUN (blood urea nitrogen)
Maintenance
phase: sustained oligouria (40-400ml/day); salt & water overload; increased
BUN; hyperkalemia; metabolic acidosis and other manifestations of uremia.
Recovery
phase: increased urine volume up to 3L/day; large loss of H2O, Na+,
K+, (causing hypokalemia); BUN and creatinine levels return to normal
Biochemical:
6.
(a) Is this condition reversible?
Yes
(b)
Does it have the same prognosis as glomerular injury?
No
<< PREVIOUS INDEX NEXT SLIDE >>
Copyright � Joseph Ong 2003