Fatty Liver
Click to see other slides: [1] [2]
1.
What are the different cell types in the liver and their distinguishing
features?
Hepatocytes:
arranged in chains between which lies sinusoids, which drain into the central
vein of lobule.
Blood
vessels and corresponding cell types.
Kuppfer
cells: these are typical macrophages found within sinusoids.
2. Which vascular beds do the central veins derive their blood flow?
Sinusoids,
draining the hepatic portal vein and hepatic artery.
3. What is the difference between the lobule concept and the acinus concept
of liver?
Classic
liver lobule:
� Classic liver lobule has a central vein (CV) as
the axis of the hexagonal lobule, while the 6 corners of the hexagon are the
portal triads
� Blood flows from periphery to centre of classic
liver lobule. Oxygen and metabolites, toxic and non-toxic substances absorbed in
the intestines reach the periphery cells first before the CV.
Portal
lobule:
� Portal lobule has at its centre the portal triad
(PT) and its periphery the regions of adjoining hepatic lobules.
� Is triangular.
Has CV at the tips of each of its angles. Contains parts of 3 adjoining liver lobules.
Hepatic
acinus:
� Diamond shaped.
Is region irrigated by a single distributing vein.
Is situated in adjacent areas of 2 liver lobules.
� Based in proximity to distributing veins, cells
in the hepatic acinus area divided into 3 zones.
� Zone I : closest, thus 1st to alter incoming
blood or be affected by it
� Zone II : next to respond
� Zone III : portal vein blood that has already
been altered by cells in zone I and II.
� Zonal arrangement accounts for why there is
difference in selective damage of hepatocytes caused by various noxious agents
or disease conditions.
4. What are some physiologic consequences of functional zonation in the
liver?
The
hepatocytes that are nearest to the portal triad receives the most blood supply
and are least susceptible to ischemia while those at the central veins are the
most susceptible. Thus
microvesicular fat droplets usually appears first in hepatocytes around the
central veins. Functional zonation
allows for the surgical removal of an affected part of the liver without
affecting other parts.
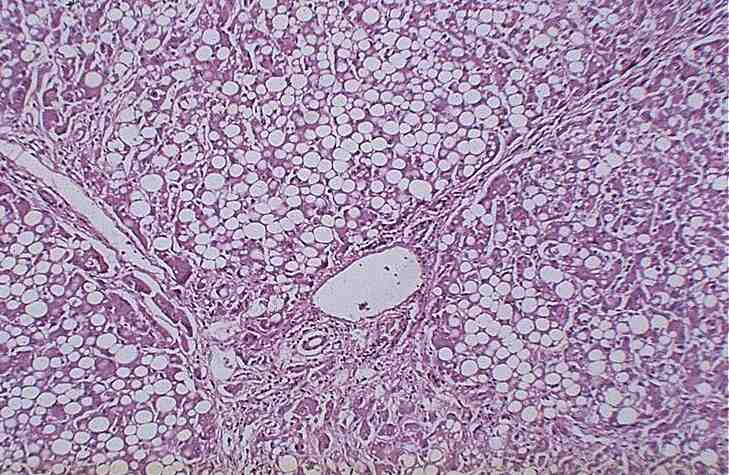
5. What histopathologic features are present on the slide?
Fat
vacuoles in hepatocytes, nucleus displaced to periphery of cell (macrovesicular
steatosis).
The
architecture is not disruptive and fatty cysts may be seen.
What
is the gross appearance of the liver?
Greasy,
slightly yellow, enlarged (fatty liver).
6. How would you demonstrate the contents in the vacuole?
By
special staining techniques e.g. with Sudan Red and Oil red O.
Frozen tissue sections of either fresh or aqueous formalin must be used.
Do not use alcohol or any stains containing lipid solvents.
7. What condition is represented here?
Fatty
change.
8. How did those vacuoles form?
Vacuoles
in the liver may contain fat, water or polysaccharides such as glycogen.
In this case the vacuoles contain fat.
Formation
of those vacuoles is by excess accumulation of triglycerides within liver
hepatocytes.
This
results from defects in any one of the steps of normal fat metabolism by the
liver.
These
steps are:
1. uptake of free fatty acids by liver hepatocytes
2. esterification of free fatty acids to triglycerides
3. packaging of triglycerides with apoproteins to form lipoproteins
4. release of lipoproteins into circulation
9. Name some common causes.
1. Secrease
secretion of triglycerides (defective apo B 100)
2. Microsomal damage due to alcohol via acetaldehyde
3. CCl4
and protein malnutritiondecrease synthesis of apo proteins.
4. Hypoxia
5. Diabetes mellitus.
6. Obesity.
10.
Is this condition reversible?
Yes.
Copyright � Joseph Ong 2003