What is it like to be banded?
How much can you eat? How
fast do you lose weight? What are the negative
side-effects? Are there foods you can't eat?
Are there any risks?
Do you miss eating large amounts of food? What
about exercise? How hard was it to make the mental
and physical adjustments? How much does it cost?
Is the band forever? What about sweets?
Discovering the Band
How did you hear about the band?
My friend Robin first introduced me to the band in the summer
of '99. She confided in me that she too was sick of being overweight, and
after researching all the WLS options, she decided the band was for her. Took
me several days of soul-searching to realized that I wanted to lose weight
too.
Why did do choose the band? -- See "Why
the Band?"
How did you do your research?
I followed a few links Robin sent my way and joined the Bandsters
group. From there I got in touch with alot of banded people and asked them
their experiences. With time I started searchin on OVID and the NIH websites
for clinical studies -- most studies are published in the Obesity Surgery
journal. Abstracts of many recent studies are available on the Bandsters'
file section -- for members only.
My best suggestion is to join Bandsters and search their websites
and the member websites for detailed information
Good online support groups?
Well, of course Bandsters
is the best place to start. It's an international list of people in all stages
of the AGB process. We have long-timers and people investigating the band.
We have Swedish (SAGB) and Lap-Band patients, and people who have travelled
abroad for surgery.
The list is rather large (300+ as of the summer of 2000), and
the volume can be high. I recommend that unless you are willing to deal with
20-40 messages a day, that you stick to the Digest or Web-Only versions. To
subscribe, go to http://www.egroups.com/group/Bandsters.
There are other specialized lists, usually by region, that might
be more useful to certain people. These include:
Do know that most of these lists are much less active than the main Bandster
list and might not have the depth of information available. I recommend that
people at least join Bandsters through a Web-Only subscription, so that they
have access to private files and can post questions when needed.
top
General Band Questions
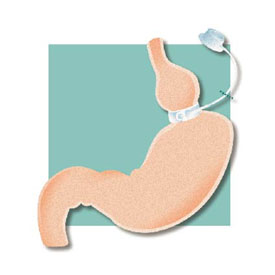
How does the band work?
|
The band, placed around the outside of the stomach, draws
itinto an hourglass shape with a small upper pouch for food. This pouch
gets full with very little food, leaving the patient content with much
less. The food then slowly works through the hourglass and into the
lower part of the stomach. From there the food is digested normally.
No changes are made to the digestive system and the stomach is not
cut or stapled.
The band can be adjusted by injecting saline into the
subtanceous port, which then goes through the tubing to inflate the
balloon.
The port is either attached to the sterum or imbedded
in the lower-left side of the abdomen.
|
|
What are the risks involved?
Risks include:
I'm in the process of compiling complications rates of the band, but they are
generally in the 0-10% range (mostly minor slippage or infection) and are lower
with well-trained and experienced surgeons. The most common complications are
small slippages of the band -- usually treated by emptying the band of fluid
and letting the stomach slip back into place. Although a few patients have needed
a reoperation because of misplaced or slipped bands, this is extremely rare.
Find a competent and well respected surgeons and these risks become extremely
small.
Can the band slip or break?
Yes -- slippage can happen, but very rarely requires re-operation.
I've never heard of a band breaking or bursting inside a patient, although
I suppose it's possible. But these bands are designed to hold many times more
liquid than will every be injected clinically.
What is the difference between the Swedish and Lap-Bands®?
Very little. Swedish bands have a bigger clinical capacity (9
to 11 mls) verus the Lap-Band® which is rarely filled over 5.0 mls. The
SAGB is considered a low-pressure band, although I'm not sure what difference
that has in complication rates or patient experience. On the Bandsters list,
the only time these differences come up is when talking about fill levels.
The SAGB is routinely implanted with 3.0 mls already filled,
while the Lap-Band is rarely inserted with any fill amount. At this time only
the Lap-Band® is in FDA Clinical Trials, and will probably be the only
band used in the US.
I suggest that patients trust their surgeon's opinion on which
band to use, if there is a choice. American citizens may want to give slight
perference to Lap-Bands® as they will be the domestic standard -- and
will be more familiar to any fill doctor they may find locally.
top
My Procedure
Who was your surgeon?
Dr. Carlos Gracia, seen here with his Bariatric Coordinator,
Debbie.
Where did you have it done?
San Ramon Region Medical Center -- Northern California
How much did it cost?
$19,000 -- minus some insurance coverage for my gallbladder
removal and hernia repair.
Did it hurt?
The first 24 hours hurt -- but hard to tell if that is from
the gallbladder and hernia, or the band. I felt 80% better by the time I was
discharge 3 days later, and fully functional within a week.
How long were you in the hospital?
3 days, total.
What kind of pre-op tests did you need to take?
From what I can remember:
- Routine bloodwork
- EKG
- BMI and dietary evaluation
- Ultrasound to check for gallstones -- I had them, unbeknownst to me, so
they were removed.
- Barium swallow
- Extensive psychological evaluation
Were you in the FDA trials? How is that different than going
abroad?
Yes, I was in the trials. Not sure how it differs exactly, although
I suspect I had more tests, had to wait longer for nearly everything and my
results were more closely monitored. But then again, I had my surgery 20 minutes
from home with an excellent surgeon. I don't mind being in the trials, although
I paid more and have to wait longer for fills.
top
Side Effects
Do you ever feel pain?
About once a week I forget to chew well and and food can get
stuck for awhile. Ocassionally I eat one too many bites and it feels tight
in my chest. Once or twice a month I may productively burp a stuck piece of
food out.
But I rarely feel hungry, my knees don't hurt and I feel much
stronger than before. An easy trade, in my book.
Have you ever 'productively burped'?
Yes, 4 or 5 times, total. Usually because I didn't chew well,
or because I ate too quickly or too late at night.
What about slippage?
Yes, it can happen, but not to me or anyone in my surgeon's
office.
Does your port ever hurt?
For the first 2 months it was tender. Now that I've lost weight,
I can feel it more easily, and I choose not to do sit-ups because it makes
it feel sore. After I reach goal, I will have a mini-port installed, and hope
to be able to do crunchs again.
top
Food and Eating
How long were you on liquids?
Supposedly for 4 week. In reality -- 10 days. Went on soft solids
at 10 days with surgeon approval.
Do you ever diet with the band?
Sometimes I count my calories (or WW points) and make a more
proactive choice to avoid fattening foods. In that respect it's similar to
dieting. But it is different in that I rarely feel hungry, can easily stay
within any program and don't feel deprived. Even at my most conscientious,
I still eat whatever I want, if the spirit truly moves me. But after taking
a second and asking myself if I really want the food, I usually don't.
Once restricted, people lose weight without consciously chosing
'good food', but it might be slower than if they decided to diet. Before getting
good restriction (1-3 fills), food choice will play a bigger part in weight
loss. Of course, actively subverting the band with chocolate or hi-cal liquids
will stall weight loss.
If you want to lose faster, then pay more attention to the food
you eat. But if dieting is too tough or mentally draining, then make sure
you get properly restricted and stop eating when full. The eventual goal is
a healthy and normal relationship with food -- which means getting out of
the diet mentality. But this also means picking the best fuel possible for
your body -- and that means fresh veggies and fruit and lower fat proteins.
Each person comes to their own balance.
How much can you eat in one meal?
It varies with the level of restriction. See my stages
page...
Are you stuck with only soft foods?
No! In fact, I recently had a steak for dinner -- filet mignon,
medium rare. Took tiny bites and stopped when full -- probably had 1-2 oz
total, over a 45 minute period. Some people find that soft foods are easier
to deal with, and a few people can't tolerate specific items like bread or
rice. Personally, I can eat whatever I want, if I do it slowly and chew well.
Are there foods you can't eat?
More than a bite of bread fills me, so I keep that for special
occassions. Eating late at night isn't a good idea, and I prefer liquids in
the morning. But so far, there isn't a single thing sworn off my menu -- just
food that takes so long to chew that it doesn't seem worth it.
Is it possible to subvert the band?
Yes, by eating or drinking hi-calorie liquid or soft foods.
An occasional scoop of ice cream will not undo your good work, but a daily
milkshake and candy bar can throw you behind.
top
Fills
What is a fill?
(taken from the glossary): A syringe
injection of saline or similar substance into the submuscular port in order
to increase the pressure of the band around the stomach. This is the process
that allows patients to adjust the pressure of the band, thereby affecting
how much food they are able to eat and how quickly the food drops into the
lower stomach. Fills are usually first given 4-8 weeks post-op, but can occur
sooner or later as the surgeon and patient see fit. Most patients find that
they need several fills before feeling a significant level of restriction.
A surgeon or fill technician may or may not require a fill to be done under
fluroscopy.
When do people get their first fill?
4-12 weeks post-op.
How much do you get in your first fill?
I haven't lost weight in several weeks? Do I need another fill?
First check to see if you are following the 7
Golden Rules of AGB -- you should be following these rules to the best
of your ability. If after 3 weeks and honest work at following these rules,
if the plateau has not been broken, the go in for a fill.
top
"What is that Sensation?"
After a few bites it feels like someone is stepping on my chest/stabbing
me in the chest.
During the first few weeks on solids, it may feel like every
meal produces a tightness in the chest. This is pretty normal -- it's the
full feeling that the band provides. Take this as a signal to stop eating.
With time and practice these feelings will subside and you will re-learn how
to eat smaller bites and stop before it gets too much.
You can also try going back on liquids for a few hours and see
if that alleviates the pain. If you have pain after every meal or indigestion
before meals, please contact your surgeon.
About 10 minutes after eating I get this intense pain between
my breasts, like something is stuck.
Something probably is stuck. You didn't chew well enough --
common mistake, especially early on. In all likelihood, the feeling will go
away in a few minutes, either with the food passing through the stoma, or
coming back up. If things get horrible, try several of the common tricks to
induce a productive burp -- drinking warm salt water, drinking a mixture of
warm water and meat tenderizer, or a small sip of carbonated soda. Once the
food comes up or passes through, the pain will fade away.
I can't seem to swallow my spit -- what's happening?
Something is stuck. See above.
About 10 minutes after I eat, I can feel my food passing through
the stoma, but it's not painful. Is that normal?
This is pretty normal, especially after fill.
If I eat before going to bed, I wake up with terrible heart-burn
and sometimes coughing.
This is probably acid reflux, and if it isn't solved with the
following recommendations, you may be overfilled and need to have a small
amount removed. Try the following common recommendations:
-
-
Flush out the stoma by drinking some water an hour before bed
-
Sleep with the head of the bed slightly evelated
-
OTC heart-burn medication, such as Mylanta, Pepcid AC or Tagament can reduce
pain.
top
Weight loss
How quickly will I lose weight with the band?
The standard weight loss is 1-2 pounds per week, on average.
I've lost an average of 7-10 pounds per month.
Will I lose as much with AGB as I would with an RNY or VBG?
Studies vary on this, but the evidence seems to say that these
traditional WLS will produce faster weight loss, but after 18-24 months,
the weight loss seems to even out. AGBers also do not face the same rates
of complications, nor do they have as big of a bounceback (regain of weight
after getting to goal), because the band can be adjusted to suit the individual.
Will have to go through the research, but I remember the ILOST
page having information about this.
How much do people lose on the liquid stage?
It varies widely, some only lose a few pounds, some lose quite
a bit (20-40 pounds). It depends on several factors including starting weight,
length of liquid stage, etc. I lost 6 pounds during my hospitalization and
10 day liquid stage.
Will my weight loss plateau once I'm off liquids but before
my first fill?
It may. You may even gain a pound or two back. This will be
rectified once you get a fill. Since I had to wait 3 months for my first fill,
I decided to do some gentle dieting, and lost another 21 pounds before getting
my fill.
I haven't lost weight in over a month. How can I break my plateau?
-
-
Follow a strict diet plan -- I've seen ones that advocate
nothing but protein (6 2 oz servings per day) and no-cal liquids.
- Get a fill.
How much should I expect to lose after a fill?
top
Exercise
Can I exercise with the band?
Yes, after the initial healing period.
Are there moves or activities that I won't be able to do after
banding?
Not specifically, but I'd check with your surgeon if you wanted
to play a contact sport. If you become a competetive athlete, you may want
your band loosened a tiny bit to make sure you can get adequate nutrition.
Must I exercise?
You don't have to do anything. But regular, gentle exercise
-- walking, biking, swimming -- are strongly recommended.
My port site hurts when doing some activities. What are my
options?
- Don't do that activity.
- Talk to your surgeon about getting a mini-port or having the port removed
-- usuall yonly done when the patient is at goal.
Can I scuba-dive with my band?
Yes.
top
Tips on Working the Band
**Under construction**
top