Authors: Paolo Vinci M.D. and Sandra Linet Perelli M.D.
Specialists in Physical Medicine and Rehabilitation at the Specialized Physiatric Hospital "L.Spolverini" Ariccia (Rome) - Italy
******PLEASE READ Disclaimer and Privacy Policy******
**Text Only and Version For Printing ** In mild cases, the tibialis anterior and the peroneal muscles are not too weak and with the help of the more preserved long extensors, will ensure sufficient dorsiflexion of the feet. In these cases, there might be tripping after prolonged walking, due to fatigue. There also may be ankle sprains, due to both altered proprioception and impaired muscular response, on uneven ground. High sport shoes, with an air chamber in the heel, are recommended for daily use because they are light, prevent ankle sprains and absorb shocks caused by the heavy gait. Foot orthoses with supports on the lateral side are helpful to reduce turning of the feet. In moderate and severe cases of CMT,the gait is characterized by footdrop, which alters phases 2 and 3 of the gait and causes increased lifting of the knee, as shown in figure n.1, where it is compared with normal gait. This altered gait is tiring, makes tripping easier, and increases the risk of falls. Up until now footdrop could be corrected only by AFOs Although AFOs are effective in correcting footdrop, there is poor acceptance of this kind of orthoses, expecially among young people and people who are conscious of their appearance with others.(eg: people who wish to wear shorts in summer, or females who prefer dresses and skirts.) A recent survey reveals that about 40% of people with CMT do not wear the prescribed AFOs and often fall or have to reduce mobility, i.e. do not walk on uneven ground or get easily tired (as they have to lift the thigh more than normal, to compensate for the inability to dorsiflex the foot). If asked, they justify their refusal with the discomfort caused by AFOs on the skin, especially in summer, when there is sweating. But the real problem of AFOs is their lack of esthetics,as they stick out of the shoes and reach the middle of the calf or the proximal part of the legs. AFOs and psychological problems for everybody with CMT, especially to adolescents, as they alter their physical self-image and reinforce the sensation of disease and disability. There are people who undergo long and painful surgical treatment, risking worsening of their CMT due to prolonged immobilization, in order to avoid AFOs, and be able to wear normal shoes. To conclude, we can say that giving the patients with CMT a totally in-shoe device to correct footdrop can help to manage their disability in a better way. "The Problem of Acceptance of AFO's in CMT" © 1998 by Paolo Vinci M.D. and Sandra Linet Perelli M.D. is on this website at the author's request. All Rights Reserved
This Website was created and is maintained by Webmaster Email: D.B. Gosling

and the Medinex Code Of Online Excellence
![]()
The Gait
Normal Gait
CMT Gait
Foot Drop In CMT
AFOs in CMT
Our Solution
The Device
CMT Foot Without Device
CMT Foot WIth The Device
Examples Of Shoes Suitable For Modification
Pictures From Video Tape
![]()
![]()
![]()
![]()


![]()
Normal Gait
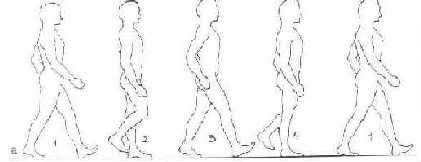
Phase 1
Phase 2
Phase 3
Phase 4
Phase 1
![]()
CMT Gait
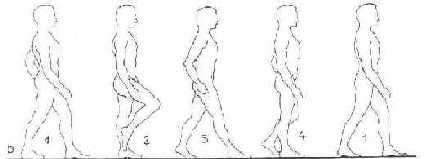
Phase 1
Phase 2
Phase 3
Phase 4
Phase 1
![]()
Click on the IMAGE for a larger view and

use the back button on your browser to return here
![]()
![]()
![]()
![]()


Dorothy B. Gosling (Retired R.N.)
All rights reserved © Copyright 1997-2005 ![]()
The Views & Opinions of Contributors To This Website are not necessarily shared by the Webmaster
Disclaimer and Privacy Policy Some Web Page Design features have been supplied by AT&T Canada Inc©. Others have donated their time, money and expertise for the benefit of all CMTers. It is also privately funded by the Webmaster.
Changes last made on:Tuesday January 11, 2005 5:15:16 PM