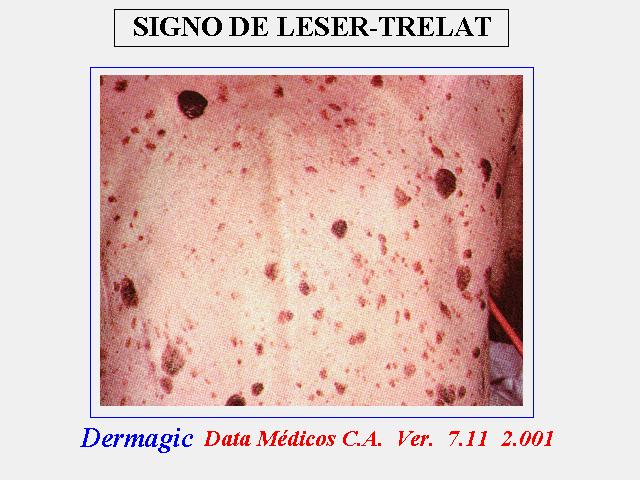
The Leser-Trelat
sign, a reality./ El signo de Leser-Trelat, una realidad.
Data-Medicos
Dermagic/Express No. 2-(92)
05 Abril 2.000 05 April 2.000
~ El Signo de Leser-Trelat, una Realidad ~
~ The Leser-Trelat Sign, a Reality ~
EDITORIAL ESPANOL
=================
Hola amigos de la red, DERMAGIC de nuevo con ustedes. El tema de hoy:
EL
SIGNO DE LESER-TRELAT. Fueron los cirujanos Edmun LESER (Aleman) y
y
Ulysse TRELAT (Francia) profesor de cirugia en Bordeaux, quienes a
finales del siglo 18 describieron por vez primera la asociacion de
tumores vasculares de la piel (angiomatosis senil) con carcinoma y
malignidad visceral. Posteriormente le correspondio a Hollander en
el
año 1.900 (hace un siglo) la primera descripcion de "verrugas
seborreicas" asociadas con cancer interno.. El describio la ocurrencia
simultanea de 1.) angiomas, 2.) maculas pigmentadas y 3.) QUERATOSIS
SEBORREICAS como un signo temprano de cancer. Los angiomas seniles
fueron los de menor significado. Posteriormente el mismo Hollander
en un
nuevo trabajo insistio en en la asociacion necesaria de los TRES TIPOS
DE LESIONES y su asociacion con malignidad y tambien en la aparicion
subita y rapido desarrollo de las lesiones. En su opinion las de mayor
significado fueron las maculas pigmentadas. Fueron posteriores
descripciones donde se encontro que la principal carateristica del
signo
son las QUERATOSIS SEBORREICAS, por ello algunos autores Descalifican
el
TERMINO LESER-TRELAT pues en la descripcion ORIGINAL NO SE HABLO NUNCA
DE queratosis seborreicas asociadas a malignidad interna.
Yo pienso que estos Autores LESER Y TRELAT se inmortalizaron en ese
siglo pues se dieron cuenta que existian marcadores cutaneos de
malignidad interna, y por ello creo que el signo LESER-TRELAT es una
realidad. Espero disfruten estas referencias.
Saludos a todos !!!
Dr. Jose Lapenta R.,,,
EDITORIAL ENGLISH
=================
Hello friends of the net, DERMAGIC again with you. Today's topic: THE
LESER-TRELAT SIGN. They were surgeons Edmun LESER (German) and
Ulysse
TRELAT (France) surgery professor in Bordeaux who at the end of the
18
th Century they described for first time the association of vascular
tumors of the skin (senile angiomatosis) with carcinoma and visceral
malignancy.
Later on it corresponded him to Hollander in the Year 1.900 (a century
ago) the first description of seborrheics warts associated with
internal cancer.. He described the simultaneous occurrence of 1.)
angiomas, 2.) pigmentary spots and 3.) SEBORRHEIC KERATOSES like
an
early sign of cancer. The senile angiomas were the least significant
of
these features. Later on the same Hollander in a new work insisted
in
the necessary association of the THREE TYPES OF LESIONS and its to
sociacion with malignancy and also in the sudden appearance and rapid
development of the skins lesions. In his opinion the pigmentary spots
where the most important. They were later descriptions where it was
found that the main characteristic of the sign is the SEBORRHEIC
KERATOSES, for it some authors Disqualify the I TERM of
LESER TRELAT
SIGN because in the ORIGINAL description ONE NEVER SPEAKS OF
seborrheic
keratoses associated to internal malignancy.
I think that these Authors LESER AND TRELAT were immortalized in that
century because they demonstrated that cutaneous markers of internal
malignancy existed, and for I believe it that the SIGN of LESER-TRELAT
is a reality. I wait you enjoy these references.
Greetings to ALL, !!
Dr. Jose Lapenta R.,,,
===================================================================
REFERENCIAS BIBLIOGRAFICAS / BIBLIOGRAPHICAL REFERENCES
===================================================================
===========================================================
1.) Coexistence of acanthosis nigricans and the sign of Leser-Trelat
in
a patient with gastric adenocarcinoma: a case report and literature
review.
2.) Sign of Leser-Trelat.
3.) Pancreatic carcinoma associated with the Leser-Trelat sign.
4.) Leser-Trelat sign with anaplastic ependymoma--an autopsy case.
5.) The sign of Leser-Trelat associated with esophageal carcinoma.
6.) Hereditary onset of multiple seborrheic keratoses: a variant of
Leser Trelat sign?
7.) Cutaneous paraneoplastic syndromes in solid tumors.
8.) Benign Leydig cell tumor of the testis associated with human
papillomavirus type 33 presenting with the sign of Leser-
9.) A case of pancreatic cancer with the sign of Leser-Trelat.
10.) The sign of Leser-Trelat: a cutaneous sign of internal malignancy:
weakened subepithelial matrix from the effect of neoplasms on the
extracellular matrix of the host.
11.) [Skin manifestation of internal malignancy].
12.) Leser-Trelat sign associated with Sezary syndrome.
13.) The sign of Leser-Trelat associated with transitional cell
carcinoma of the urinary-bladder--a case report and short review.
14.) Mycosis fungoides with Leser-Trelat sign: the first report of
a
patient from Japan.
15.) The sign of Leser-Trelat associated with adenocarcinoma of the
rectum.
16.) Seborrheic keratoses and cancer.
17.) The sign of Leser-Trelat in a young woman with
osteogenic sarcoma.
18.) Sign of Leser-Trelat with a metastatic mucinous adenocarcinoma.
19.) The sign of Leser-Trelat: does it exist? [see
20.) The sign of Leser-Trelat associated with malignant melanoma.
21.) Paraneoplastic rhinophyma and the Leser-Trelat sign.
22.) Transformation of lymphocytoma cutis into a malignant lymphoma
in
association with the sign of Leser-Trelat.
23.) Leser-Trelat sign associated with Sezary syndrome.
24.) The sign of Leser-Trelat associated with primary lymphoma of the
brain.
25.) Acanthosis nigricans and the sign of Leser-Trelat associated with
adenocarcinoma of the gallbladder.
26.) Bile duct adenocarcinoma with Leser-Trelat sign and pure red blood
cell aplasia.
27.) The sign of Leser-Trelat. Report of a case with adenocarcinoma
of
the duodenum.
28.) [The Leser-Trelat symptom: report of two cases
29.) Adenocarcinoma of the stomach with eruptive seborrheic keratoses:
the sign of Leserp-Trelat.
30.) Florid cutaneous papillomatosis, malignant acanthosis nigricans,
and pulmonary squamous cell carcinoma.
31.) The relation between seborrheic keratoses and malignant solid
tumours. A case-control study.
32.) Transformation of Sezary syndrome and the sign of Leser-Trelat:
a
histopathologic study.
33.) Sign of Leser-Trelat: report of two cases and review of the
literature.
34.) Pemphigus foliaceus resembling eruptive seborrheic keratoses.
35.) Eruptive seborrheic keratoses in a young woman with acromegaly.
36.) Seborrheic keratosis and papillomatosis: markers of breast
adenocarcinoma.
37.) A case of hepatocellular carcinoma with the sign of Leser-Trelat:
a
possible role of a cutaneous marker for internal malignancy.
38.) the relation between seborrheic keratoses and malignant solid
tumours. A case-control study.
39.) [Useful cutaneous markers of internal malignancy in the early
stage].
40.) [Gastrointestinal carcinoma with skin diseases from the standpoint
of surgery].
41.) [Leser-Trelat sign in adenocarcinoma of the sigmoid colon--a rare
clinical picture].
42.) [Acanthosis nigricans maligna and Leser-Trelat sign in double
malignancy of the breast and stomach].
43.) Beitrage Zur Fruhdiagnose des darmcarcinoms (Hereditasverhaltnisse
und Hautveranderungen)
===========================================================
===========================================================
1.) Coexistence of acanthosis nigricans and the sign of Leser-Trelat
in
a patient with gastric adenocarcinoma: a case report and literature
review.
===========================================================
J Am Acad Dermatol 2000 Feb;42(2 Pt 2):357-62
Yeh JS, Munn SE, Plunkett TA, Harper PG, Hopster DJ, du Vivier AW
Department of Dermatology, King's College Hospital, London, United
Kingdom.
The association of acanthosis nigricans (AN) with the sign of
Leser-Trelat (LT) and gastric carcinoma is rare. Our patient was a
69-year-old man, who presented with hematemesis; a stage-IV poorly
differentiated, diffuse-type, adenocarcinoma of the gastric antrum
was
diagnosed. The AN was striking, with florid cutaneous papillomatosis
that also involved the mucous membranes of the mouth and eyelids, and
keratoderma. AN and the sign of LT predated tumor detection by 6 months
and regressed after chemotherapy in parallel with reduction of the
tumor
load, demonstrating the dermatoses as paraneoplastic phenomena. The
patient died 7 months after completion of chemotherapy. The coexistence
of AN and the sign of LT should prompt a search for underlying
malignancy. The pathogenesis of both dermatoses is discussed.
===========================================================
2.) Sign of Leser-Trelat.
===========================================================
J Am Acad Dermatol 1996 Jul;35(1):88-95 Related Articles, Books, LinkOut
Schwartz RA
New Jersey Medical School, Newark 07103-2714, USA.
The sign of Leser-Trelat is rare. It is defined as the sudden eruption
of multiple seborrheic keratoses caused by a malignancy. Because both
seborrheic keratoses and cancer are common in the elderly, it is not
always easy to tell from the literature or in any given patient if
this
sign is present. In fact, its validity has been questioned. Its
association with malignant acanthosis nigricans is one of several of
its
features that support its legitimacy as a true paraneoplastic disorder.
===========================================================
3.) Pancreatic carcinoma associated with the Leser-Trelat sign.
===========================================================
Int J Pancreatol 1997 Oct;22(2):155-60 Related Articles, Books
Ohashi N, Hidaka N
Department of Surgery, Matsusaka Chuo Hospital, Mie, Japan.
A case of pancreatic carcinoma associated with the Leser-Trelat sign
is
reported. A 53-yr-old male had complained of mild epigastric discomfort
and back pain accompanied by seborrheic keratoses, which had increased
in size and number over the previous 6 mo. A tumor was detected in
the
head of the pancreas and macroscopically curatively resected. His skin
lesions diminished after surgery, but progressed again when the tumor
recurred. Immunohistology for EGF showed a low level in the pancreatic
carcinoma cells but a higher EGF content was recognized in the
hyperkeratinized portions of the seborrheic keratoses. Of 130 underlying
malignancies described in the 125 reported patients with the
Leser-Trelat sign, neoplasms of the gastrointestinal tract were most
common, comprising 47.7% of the total. The present case is the third
case showing an association between a pancreatic carcinoma and the
Leser-Trelat sign, but the first case for which the tumor of the
pancreas was diagnosed in an early stage and resected surgically, as
a
result of the suggestive nature of this sign.
===========================================================
4.)Leser-Trelat sign with anaplastic ependymoma--an autopsy case.
===========================================================
Acta Neuropathol (Berl) 1997 Jan;93(1):97-100 Related Articles, Books,
LinkOut
Hamada Y, Iwaki T, Muratani H, Imayama S, Fukui M, Tateishi J
Department of Neuropathology, Faculty of Medicine, Kyushu University,
Fukuoka, Japan.
A 36-year-old Japanese male, who 7 years previously had been diagnosed
as having an ependymoma in the left parietal region, had received
surgery, chemotherapy and radiotherapy. He later developed a rapid
growth of multiple skin lesions on his back and extremities, which
coincided with a regrowth of the tumor. Postmortem examination revealed
that the ependymoma showed anaplastic transformation and necrosis;
however, no malignancy was observed in the extracranial organs. The
skin
lesions were histologically diagnosed as seborrheic keratoses. We have,
therefore, diagnosed the patient as having Leser-Trelat sign associated
with anaplastic ependymoma.
===========================================================
5.) The sign of Leser-Trelat associated with esophageal carcinoma.
===========================================================
Am J Gastroenterol 1996 Apr;91(4):802-4 Related Articles, Books, LinkOut
Chiba T, Shitomi T, Nakano O, Shimotono H, Yamada H, Fujimaki E, Orii
S,
Sato K, Sato S
First Department of Internal Medicine, School of Medicine, Iwate Medical
University, Morioka, Japan.
A 79-year-old woman was admitted to our hospital with complaints of
dysphagia and multiple verrucous papules that had developed over the
previous year. The diagnosis of esophageal carcinoma was based on upper
gastrointestinal radiography and endoscopic examination with biopsy.
The
clinical syndrome was consistent with the sign of Leser-Trelat
associated with esophageal carcinoma. Although radiation therapy and
chemotherapy were undertaken, the patient died 8 months later because
of
the sign of Leser-Trelat in association with squamous cell esophageal
carcinoma.
===========================================================
6.) Hereditary onset of multiple seborrheic keratoses: a variant of
Leser Trelat sign?
===========================================================
J Dermatol 1996 Mar;23(3):191-5 Related Articles, Books
Yamamoto T, Yokoyama A
Department of Dermatology, Tsuchiura Kyodo General Hospital, Ibaraki,
Japan.
A 79-year-old man in a cancer-prone family developed disseminated
seborrheic keratoses over his trunk and extremities over a few decades
without rapid increase. His son, mother, and one of his brothers, who
died of gastric cancer, also had numerous seborrheic keratoses for
a
long time. He had a biliary tract cancer. Histologic examination showed
hyperproliferation of basaloid cells branching downwards, as if induced
by surrounding stroma. No decrease of the number of seborrheic keratoses
after surgical operation has been observed. Examination for the
localization of epidermal growth factor receptor (EGF-R) and HER-2/neu
oncoprotein by immunohistochemistry revealed positive staining on the
epithelial strands branching downwards on the specimens of seborrheic
keratoses. A different pattern of expression was demonstrated in normal
seborrheic keratosis. These findings suggest that some unidentified
growth factors may be involved in the induction of visceral and/or
cutaneous neoplasms in this family.
===========================================================
7.) Cutaneous paraneoplastic syndromes in solid tumors.
===========================================================
Am J Med 1995 Dec;99(6):662-71 Related Articles, Books
Kurzrock R, Cohen PR
Department of Clinical Investigation, University of Texas M.D. Anderson
Cancer Center, Houston 77030, USA.
OBJECTIVE: To provide an overview of the clinical manifestations,
pathophysiology, and oncologic implications of the cutaneous
paraneoplastic syndromes that occur predominantly in patients with
solid
tumors. METHODS: A review was performed of the literature identified
by
a comprehensive MEDLINE search. RESULTS: Diverse cutaneous
paraneoplastic syndromes may be associated with underlying tumors.
They
include musculoskeletal disorders (clubbing, hypertrophic
osteoarthropathy, dermatomyositis, and multicentric
reticulohistiocytosis), reactive erythemas (erythema gyratum repens
and
necrolytic migratory erythema), vascular dermatoses (Trousseau's
syndrome), papulosquamous disorders (acanthosis nigricans, tripe palms,
palmar hyperkeratosis, acquired ichthyosis, pityriasis rotunda, Bazex's
syndrome, florid cutaneous papillomatosis, the sign of Leser-Trelat,
and
extramammary Paget's disease), and disorders of hair growth
(hypertrichosis lanuginosa acquisita). The clinical manifestations
of
these dermatoses may precede, coincide with, or follow the diagnosis
of
cancer. The presence of a cutaneous paraneoplastic syndrome is often
associated with a poor prognosis. CONCLUSIONS: Cutaneous paraneoplastic
syndromes are specific constellations of mucous membrane and/or skin
abnormalities that are caused by an underlying tumor. Since they may
be
the presenting sign of an occult cancer, cognizance of their features
and clinical implications are of considerable importance. Individuals
with these syndromes should have a thorough workup for an associated
malignancy.
===========================================================
8.) Benign Leydig cell tumor of the testis associated with human
papillomavirus type 33 presenting with the sign of
Leser-===========================================================
Trelat.
J Urol 1993 Oct;150(4):1246-50 Related Articles, Books
Martin RW 3d, Rady P, Arany I, Tyring SK
Department of Dermatology, Johns Hopkins School of Medicine, Baltimore,
Maryland.
We present a case of a benign testicular Leydig cell tumor and eruptive
seborrheic keratosis associated with human papillomavirus type 33
infection. To our knowledge this is the first occurrence of a Leydig
cell tumor in a patient with tuberous sclerosis and the second
documented case of eruptive seborrheic keratoses (sign of Leser-Trelat)
associated with a benign neoplasm.
===========================================================
9.) A case of pancreatic cancer with the sign of Leser-Trelat.
===========================================================
Nippon Geka Hokan 1993 Jul 1;62(4):203-8 Related Articles, Books
Hirano T, Yoshioka H, Manabe T
Department of Surgery, Yoshioka Hospital, Kyoto, Japan.
A case of 79-year-old man with pancreatic cancer associated with the
sign of Leser-Trelat was presented. Abdominal CT scanning was performed
and a pancreatic tail tumor involving the spleen and the greater omentum
as well as ascitic retention were detected. Ba-enema study showed the
stenosis of the sigmoid colon, suggesting the peritoneal disseminations.
Absolute non-curative operation of side-to-side transverso-sigmoidostomy
was performed for colonic stenosis, and biopsy of the disseminated
omental tumor was performed, which was histologically diagnosed as
well
differentiated papillary adenocarcinoma compatible with pancreatic
cancer. The postoperative course was uneventful and at present the
patient was followed at outpatient clinic. To our knowledge, this case
is the first report with pancreatic cancer associated with the sign
of
Leser-Trelat in Japan.
===========================================================
10.) The sign of Leser-Trelat: a cutaneous sign of internal malignancy:
weakened subepithelial matrix from the effect of neoplasms on the
extracellular matrix of the host.
===========================================================
Med Hypotheses 1993 Jun;40(6):360-3
Stone OJ
The sudden onset of many seborrheic keratoses (SK) associated with an
internal malignancy (most commonly adenocarcinoma) is called the sign
of
Leser-Trelat. It is associated with acanthosis nigricans (AN) in 20%
of
the cases. There are marked changes in the extracellular matrix (ECM)
around tumors. Various fractions and depolymerized glycosaminoglycans
enter circulation. They can incorporate in the general extracellular
matrix. Mechanical factors present in AN produce extrusions of this
poor
quality ECM in the form of papillae and folds. The poor quality of
subepithelial extracellular matrix produces the marked epithelial
changes of acanthosis nigricans which shows hyperkeratosis,
papillomatosis, slight irregular acanthosis, and keratin material
formation. The neoplasm can produce the same qualitative changes in
the
subepithelial ECM on otherwise normal appearing skin. When the altered
same epithelial changes occur on this biologically altered skin the
result is many SK (the sign of Leser-Trelat).
===========================================================
11.) [Skin manifestation of internal malignancy].
===========================================================
Gan To Kagaku Ryoho 1991 Mar;18(3):365-70 Related Articles, Books
Nishiyama S
Department of Dermatology, School of Medicine, Kitasato University,
Sagamihara, Japan.
Relationship between malignant tumor of the internal organ and the skin
can be classified as skin metastasis of the malignant tumor,
non-specific skin manifestation of the malignant tumor and hereditary
syndrome which tends to have malignant tumor. I, however, discuss here
mainly about the non-specific manifestation of the malignant tumor
by
showing representative cases of the dermadrome. Such cases are
acanthosis nigricans, Leser-Trelat's sign, dermatomyositis, atypical
erythema, acquired ichthyosis, Sweet's disease, Weber-Christian's
syndrome, phlebitis migrans and Bazex syndrome.
===========================================================
12.) Leser-Trelat sign associated with Sezary syndrome.
===========================================================
SO - J Dermatol 1995 Jan;22(1):62-7
AU - Ikari Y; Ohkura M; Morita M; Seki K; Kubota Y; Mizoguchi
M
PT - JOURNAL ARTICLE
AB - A 74-year-old Japanese male had developed generalized erythroderma
and rapid growth of multiple verrucous lesions over the entire surface
of his face, trunk, and extremities three months before he was seen.
Histologically seborrheic keratoses were revealed. Laboratory
examinations showed peripheral leukocytosis with atypical lymphocytes
and high levels of IgE and IgG. On the basis of these clinical and
histopathologic findings, we diagnosed the patient as having
Leser-Trelat sign associated with Sezary syndrome. The erythroderma
subsided after administration of oral predonisone, and no new formations
of seborrheic keratosis were observed. However, because of subsequent
aggravation of the generalized erythroderma, we administered
chemotherapy. Six months after the initial examination, lung cancer
was
found, and the patient subsequently died of respiratory and renal
failure.
===========================================================
13.) The sign of Leser-Trelat associated with transitional cell
carcinoma of the urinary-bladder--a case report and short review.
===========================================================
SO - Clin Exp Dermatol 1994 Mar;19(2):142-5
AU - Yaniv R; Servadio Y; Feinstein A; Trau H
PT - JOURNAL ARTICLE; REVIEW (28 references); REVIEW OF REPORTED
CASES
AB - Leser-Trelat sign is defined as the sudden appearance of
multiple
seborrhoeic keratoses in association with internal malignancy. Although
75 cases have been reported to date, controversy still exists about
the
significance of this sign. The first association of the Leser-Trelat
sign with transitional cell carcinoma of the urinary-bladder is
reported.
===========================================================
14.) Mycosis fungoides with Leser-Trelat sign: the first report of
a
patient from Japan.
===========================================================
SO - J Dermatol 1994 Mar;21(3):189-93
AU - Miyako F; Dekio S; Tamura H; Yamada Y; Miyata N; Jidoi J;
Tohgi K
PT - JOURNAL ARTICLE
AB - We describe here a 35-year-old Japanese woman with mycosis
fungoides (MF) who developed numerous, rapidly-growing, seborrheic
keratoses on the front of her neck and chest. To the best of our
knowledge, this is the first reported case of MF with Leser-Trelat
sign
from Japan.
===========================================================
15.) The sign of Leser-Trelat associated with adenocarcinoma of the
rectum.
===========================================================
SO - Cutis 1993 Apr;51(4):255-7
AU - Cohn MS; Classen RF
PT - JOURNAL ARTICLE
AB - The authors report a case of the sign of Leser-Trelat occurring
in
a patient with primary adenocarcinoma of the rectum. The patient
demonstrated the sign several months before the internal malignancy
was
discovered. Although the majority of patients with the sign have an
underlying adenocarcinoma of the gastrointestinal tract, relatively
few
cases have been reported with the rectum as the primary site. This
case
demonstrates a classic example of the sign of Leser-Trelat and
illustrates its importance as a marker of underlying malignancy.
===========================================================
16.) Seborrheic keratoses and cancer.
===========================================================
SO - J Am Acad Dermatol 1992 Jun;26(6):947-50
AU - Lindelof B; Sigurgeirsson B; Melander S
PT - JOURNAL ARTICLE
AB - BACKGROUND: The eruptive appearance of numerous seborrheic
keratoses, the sign of Leser-Trelat, has been regarded as a reliable
cutaneous marker of internal malignancy. OBJECTIVE: We have evaluated
the possible association of malignant disease and the sign in 1752
consecutive cases of seborrheic keratoses. METHODS: First, the Swedish
Cancer Registry was searched for records of malignancies in the study
population (1958 to 1984), and the expected number of malignancies
was
calculated. Second, records of persons with malignancy within 1 year
before or after the diagnosis of seborrheic keratosis were checked
for
the sign of Leser-Trelat. Third, a case control study was performed
to
evaluate the possibility of eruptive seborrheic keratoses among the
noncancer patients in the study population. RESULTS: The results showed
a slight increased risk of cancer in the study population (relative
risk
= 1.2; 95% confidence interval = 1.0 to 1.3), mainly because of an
increased risk of cutaneous squamous cell carcinoma. In 62 patients
with
seborrheic keratoses, a malignancy (excluding skin) was diagnosed within
1 year before or after the diagnosis of seborrheic keratosis. Of these
62 patients, 6 were regarded as possibly having presented with the
sign
of Leser-Trelat. For every one of the 62 cases with seborrheic keratosis
and malignancy within one year, an age- and sex-matched control patient
without cancer was selected from the study population and the records
were checked for sudden and eruptive seborrheic keratoses. Among the
control patients, five were regarded as possibly having presented with
the sign of Leser-Trelat. CONCLUSION: This study gives no evidence
to
support the opinion that eruptive seborrheic keratoses are related
to
internal cancer risk.
===========================================================
17.) The sign of Leser-Trelat in a young woman with
osteogenic sarcoma.
===========================================================
SO - J Am Acad Dermatol 1992 Feb;26(2 Pt 2):344-7
AU - Barron LA; Prendiville JS
PT - JOURNAL ARTICLE
AB - The sign of Leser-Trelat refers to a sudden increase in
size and
number of seborrheic keratoses associated with internal malignancy.
The
validity of this cutaneous sign continues to be debated, particularly
because of the prevalence of both seborrheic keratoses and malignancy
in
the elderly population. Preceding inflammatory skin conditions are
known
to precipitate eruptions of seborrheic keratoses in otherwise healthy
persons. These cutaneous lesions may also be associated with other
markers of underlying malignancy such as acanthosis nigricans. We
present a young female patient with osteogenic sarcoma in whom eruptive
seborrheic keratoses developed. We believe this case is representative
of the sign of Leser-Trelat.
===========================================================
18.) Sign of Leser-Trelat with a metastatic mucinous adenocarcinoma.
===========================================================
SO - Cutis 1991 Apr;47(4):258-60
AU - Schwartz RA; Helmold ME; Janniger CK; Gascon P
PT - JOURNAL ARTICLE
AB - We describe a middle-aged woman with the sudden onset of
multiple
seborrheic keratoses in association with a metastatic mucinous
adenocarcinoma to the liver from an unknown primary neoplasm. This
case
illustrates the significance of the sign of Leser-Trelat and its
association with cancer.
===========================================================
19.) The sign of Leser-Trelat: does it exist? [see
===========================================================
comments]
SO - J Am Acad Dermatol 1989 Jul;21(1):50-5
AU - Rampen HJ; Schwengle LE
PT - JOURNAL ARTICLE; REVIEW (51 references); REVIEW OF REPORTED
CASES
AB - The sign of Leser-Trelat is usually regarded as a reliable
cutaneous marker of internal malignancy. We have reviewed the literature
and conclude that the evidence for a causal relation between eruptive
seborrheic keratoses and cancer is meager.
===========================================================
20.) The sign of Leser-Trelat associated with malignant melanoma.
===========================================================
SO - Cutis 1989 Jul;44(1):39-41
AU - Fanti PA; Metri M; Patrizi A
PT - JOURNAL ARTICLE
AB - A case of the sudden appearance of multiple pruritic seborrheic
keratoses (Leser-Trelat sign) associated with cutaneous malignant
melanoma is reported. To the authors' knowledge, this association has
not been previously reported.
===========================================================
21.) Paraneoplastic rhinophyma and the Leser-Trelat sign.
===========================================================
SO - Clin Exp Dermatol 1989 May;14(3):253-5
AU - Mayou SC; Benn JJ; Sonksen PH; Black MM
PT - JOURNAL ARTICLE
AB - A case of the Leser-Trelat sign associated with an underlying
malignant haemangiopericytoma is described. In addition, the patient
had
profound hypoglycaemia and a rhinophyma-like nasal swelling which
rapidly resolved post-operatively. The tumour appeared to be secreting
a
factor(s) which cross-reacted with both insulin receptors to induce
hypoglycaemia and epidermal growth factor receptors inducing a profusion
of eruptive seborrhoeic warts. It aslo had marked sebotrophic activity.
The association of the Leser-Trelat sign with malignant
haemangiopericytoma has not previously been described.
===========================================================
22.) Transformation of lymphocytoma cutis into a malignant lymphoma
in
association with the sign of Leser-Trelat.
===========================================================
SO - Acta Derm Venereol 1987;67(2):172-5
AU - Halevy S; Sandbank M
PT - JOURNAL ARTICLE
AB - A patient is described in whom transformation of lymphocytoma
cutis (LC) into malignant lymphoma, diffuse, mixed small and large
lymphocytes, occurred in association with the sign of Leser-Trelat
(LT),
which is a marker for internal malignancy. To the best of our knowledge,
such an association has not been reported previously.
===========================================================
23.) Leser-Trelat sign associated with Sezary syndrome.
===========================================================
SO - Cutis 1985 Nov;36(5):409-10
AU - Horiuchi Y; Katsuoka K; Tsukamoto K; Takezaki S
PT - JOURNAL ARTICLE
AB - The Leser-Trelat sign is a rare but well known cutaneous
indicator
of internal malignancy, most commonly adenocarcinoma of the stomach.
There have been only a few cases associated with lymphoproliferative
malignancies. Sezary syndrome is a chronic leukemia/lymphoma
characterized by generalized erythroderma and circulating Sezary cells.
We describe a rare case of the Leser-Trelat sign associated with the
Sezary syndrome. The skin sign was alleviated through combination
chemotherapy.
===========================================================
24.) The sign of Leser-Trelat associated with primary lymphoma of the
brain.
===========================================================
SO - Cutis 1984 Aug;34(2):164-5
AU - Kaplan DL; Jegasothy B
PT - JOURNAL ARTICLE
AB - The sign of Leser-Trelat has been defined as the sudden
appearance
of seborrheic keratoses in number and/or size in association with an
underlying malignancy. There have been only thirty-two reported cases
of
the sign of Leser-Trelat since it was first described in 1984. This
is
the first known case of primary lymphoma of the brain associated with
this sign. Until Dantzig's review of the literature in 1973, the only
tumor type associated with this sign had been adenocarcinomas of the
gastrointestinal tract and the genitourinary tract. Since that time
there have been only nine cases reported that were not adenocarcinomas;
of those, only four cases have been lymphoproliferative malignancies.
We
wish to emphasize the need for further reports of this sign to better
characterize it and to make physicians more aware of the association
between this dermatologic sign and an internal malignancy.
===========================================================
25.) Acanthosis nigricans and the sign of Leser-Trelat associated with
adenocarcinoma of the gallbladder.
===========================================================
SO - Cancer 1981 Jul 15;48(2):325-8
AU - Jacobs MI; Rigel DS
PT - JOURNAL ARTICLE
AB - A case of adenocarcinoma of the gallbladder associated with
acanthosis nigricans and the sign of Leser-Trelat is presented. The
significant underrepresentation of adenocarcinoma of the gallbladder
in
association with malignant acanthosis nigricans is noted. If malignant
acanthosis nigricans is caused by an ectopic peptide, a relative lack
of
production of the postulated substance by gallbladder adenocarcinoma
cells could account for this finding.
===========================================================
26.) Bile duct adenocarcinoma with Leser-Trelat sign and pure red blood
cell aplasia.
===========================================================
SO - Cancer 1980 Oct 1;46(7):1657-60
AU - Lee CH; Clark AR; Thorpe ME; Mackie BS; Firkin FC
PT - JOURNAL ARTICLE
AB - A case of adenocarcinoma of the bile duct complicating
longstanding ulcerative colitis and associated with the rapid onset
and
growth of multiple seborrheic keratosis (Leser-Trelat sign) and pure
red
blood cell aplasia is described. This is the first report of a case
of
the coexistence of the Leser-Trelat sign and pure red blood cell aplasia
in a patient with a malignancy. Both manifestations have been doubted
as
truly paraneoplastic manifestations because of their rarity in clinical
medicine. Their co-existence in the present case would support their
associaton with malignancy.
===========================================================
27.) The sign of Leser-Trelat. Report of a case with adenocarcinoma
of
the duodenum.
===========================================================
SO - Arch Dermatol 1980 Sep;116(9):1059-60
AU - Curry SS; King LE
PT - JOURNAL ARTICLE
AB - The sign of Leser-Trelat is a rare cutaneous manifestation
of
internal malignancy. Although adenocarcinoma is the most common
malignant neoplasm associated with the sign of Leser-Trelat, we report
what we believe to be the first case of adenocarcinoma of the duodenum
associated with this sign. Because of the location of the tumor, we
considered the possibility that the skin changes may be due to increased
levels of epidermal growth factor (EGF) in this patient. However, no
alteration in urine EGF levels was found.
===========================================================
28.) [The Leser-Trelat symptom: report of two cases
===========================================================
(author's transl)]
SO - Ann Dermatol Venereol 1980;107(11):1035-41
AU - Lambert D; Fort M; Legoux A; Chapuis JL
MC - English Abstract
PT - JOURNAL ARTICLE; REVIEW (22 references)
AB - The sudden occurrence and rapid increase in size and number
of
seborrheic keratoses is considered to be a symptom of internal
malignancy. But many authors did not fully agree with this finding.
We
report two cases respectively associated, the first with a mycosis
fongoides, the second with a bronchial squamous cell carcinoma. These
observations are compared with thin cases previously published in the
dermatological literature (13 patients). According to Dantzig the
commonest associated malignancy is an adenocarcinoma, and the most
frequent site the stomach. But there are also report of acute leukemia,
mycosis fongoides, Sezary and lymphocytic lymphoma. The mechanism of
the
simultaneous growth of the lesions remains unknown and may be purely
coincidental. Other case reports and several criteria still to be
defined are needed before we accept this symptom as a malignancy marker.
===========================================================
29.) Adenocarcinoma of the stomach with eruptive seborrheic keratoses:
the sign of Leserp-Trelat.
===========================================================
SO - Cancer 1980 May 1;45(9):2434-7
AU - Sperry K; Wall J
PT - JOURNAL ARTICLE
AB - The sign of Leser-Trelat, the sudden appearance of multiple
seborrheic keratoses in conjunction with an internal malignancy, is
very
uncommon. A case involving a patient who had undergone resection of
an
adenocarcinoma of the sigmoid colon followed ten years later by the
development of an adenocarcinoma of the stomach with exhibition of
the
sign of Leser-Trelat is presented. A summary of reported cases, along
with a discussion of the sign, is provided. This is the first reported
case of a patient presenting with the sign of Leser-Trelat along with
a
second primary malignancy.
===========================================================
30.) Florid cutaneous papillomatosis, malignant acanthosis nigricans,
and pulmonary squamous cell carcinoma.
===========================================================
SO - Int J Dermatol 1991 Mar;30(3):193-7
AU - Gheeraert P; Goens J; Schwartz RA; Lambert WC; Schroeder
F;
Debusscher L
PT - JOURNAL ARTICLE; REVIEW (25 references); REVIEW OF REPORTED
CASES
AB - A 72-year-old man had florid cutaneous papillomatosis (FCP),
which
is an obligatory paraneoplastic syndrome always associated with an
internal malignancy. The cancer, which is usually intraabdominal and
most often gastric in origin, evolves parallel to the FCP. This patient
is the first case of FCP occurring in association with a lung
malignancy. An association of FCP with other signs of internal cancer
is
common, with malignant acanthosis nigricans usually appearing many
times
with the sign of Leser-Trelat. FCP, malignant acanthosis nigricans,
and
the sign of Leser-Trelat are part of a continuum, developing by a common
or similar pathogenic pathway due to an underlying malignancy producing
a factor possibly similar to human epidermal growth factor.
===========================================================
31.) The relation between seborrheic keratoses and malignant solid
tumours. A case-control study.
===========================================================
SO - Acta Derm Venereol 1991;71(2):166-9
AU - Grob JJ; Rava MC; Gouvernet J; Fuentes P; Piana L; Gamerre
M;
Sarles JC; Bonerandi JJ
PT - JOURNAL ARTICLE
AB - In order to establish whether or not here is an association
between cancer and intense growth of seborrheic keratosis, the so-called
Leser-Trelat sign, we conducted a case control study in which the number
and features of seborrheic keratosis in 82 patients with recent solid
tumours, were compared with 82 age- and sex-matched controls. Neither
numbers nor features of seborrheic keratosis differed significantly
in
patients and controls. Eruptive seborrheic keratosis was noted in only
one patient and one control. This study showed that solid malignancies
are not generally associated with an increase in the number or size
of
seborrheic keratosis lesions, thus suggesting that they are not
controlled by a hypothetical secretion of growth factors by tumours.
Our
results suggest that Leser-Trelat is either a coincidence, or at most
a
very rare sign of unusual types of cancer. We also showed that multiple
cherry angiomas, previously reported to be a paraneoplastic sign, are
not regularly associated with solid tumours.
===========================================================
32.) Transformation of Sezary syndrome and the sign of Leser-Trelat:
a
histopathologic study.
===========================================================
SO - J Am Acad Dermatol 1990 Sep;23(3 Pt 1):520-2
AU - Wieselthier JS; Bhawan J; Koh HK
PT - JOURNAL ARTICLE
===========================================================
33.) Sign of Leser-Trelat: report of two cases and review of the
literature.
===========================================================
SO - J Am Acad Dermatol 1984 Jan;10(1):83-8
AU - Venencie PY; Perry HO
PT - JOURNAL ARTICLE
AB - The sudden appearance of multiple seborrheic keratoses in
the two
patients could be related to adenocarcinoma of the breast. Despite
other
isolated reports, this disorder is still controversial as a marker
of
malignancy.
===========================================================
34.) Pemphigus foliaceus resembling eruptive seborrheic keratoses.
===========================================================
SO - Arch Dermatol 1980 Jul;116(7):815-6
AU - Bruckner N; Katz RA; Hood AF
PT - JOURNAL ARTICLE
AB - A 78-year-old man had an acute eruption of lesions that
clinically
resembled seborrheic keratoses. Microscopic examination of the lesions
indicated acantholysis and dyskeratosis primarily in the granular layer.
The patient's serum contained antibodies to intercellular substance.
Direct immunofluorescence microscopy of a lesion demonstrated
immunoglobulin deposition in the intercellular areas. Treatment with
oral prednisone produced rapid resolution of the lesions. Patients
in
whom eruptive seborrheic keratoses (Leser-Trelat sign) develop should
have histological examination of their lesions to rule out the diagnosis
of pemphigus foliaceus.
===========================================================
35.) Eruptive seborrheic keratoses in a young woman with acromegaly.
===========================================================
SO - J Am Acad Dermatol 1990 Nov;23(5 Pt 2):991-4
AU - Kilmer SL; Berman B; Morhenn VB
PT - JOURNAL ARTICLE
AB - The sign of Leser-Trelat, or eruptive seborrheic keratoses,
is
purported to be a cutaneous marker for many underlying malignancies.
Elevation in levels of growth factors has been postulated to be the
stimulus for the sudden eruption of multiple new seborrheic keratoses.
In support of this hypothesis we present a case of eruptive seborrheic
keratoses in a young woman with acromegaly and elevated levels of growth
hormone.
===========================================================
36.) Seborrheic keratosis and papillomatosis: markers of breast
adenocarcinoma.
===========================================================
SO - Cutis 1983 Aug;32(2):161-2
AU - Friedman-Birnbaum R; Haim S
PT - JOURNAL ARTICLE
AB - Seborrheic keratosis (Leser-Trelat sign) and extensive florid
papillomatosis of the skin and the mucous membranes of the nose, mouth,
throat, and external genitalia were associated with adenocarcinoma
of
the breast in a 61-year-old woman.
===========================================================
37.) A case of hepatocellular carcinoma with the sign of Leser-Trelat:
a
possible role of a cutaneous marker for internal malignancy.
===========================================================
Jpn J Med 1991 Jan-Feb;30(1):53-6 Related Articles, Books, LinkOut
Tajima H, Mitsuoka S, Ohtsuka E, Nakamura Y, Nakayama T, Satoh Y, Shima
M, Nakata K, Kusumoto Y, Koji T, et al
First Department of Internal Medicine, Nagasaki University School of
Medicine, Japan.
A rare case of hepatocellular carcinoma who developed the complication
of the sign of Leser-Trelat is reported. The patient, a 57-year-old
male, visited our hospital with complaints of generalized malaise and
anorexia. A diagnosis of hepatocellular carcinoma was made based on
elevated alpha-fetoprotein measurement, ultrasonography, and hepatic
arteriography findings. Chest x-ray film suggested pulmonary metastases
of hepatocellular carcinoma. Thereafter, complications of the seborrheic
keratosis developed in the trunk and the skin lesion was diagnosed
as
the sign of Leser-Trelat associated with hepatocellular carcinoma.
The
patient died of pneumonia 9 months after development of the sign of
Leser-Trelat.
===========================================================
38.) the relation between seborrheic keratoses and malignant solid
tumours. A case-control study.
===========================================================
Acta Derm Venereol 1991;71(2):166-9 Related Articles, Books
Grob JJ, Rava MC, Gouvernet J, Fuentes P, Piana L, Gamerre M, Sarles
JC,
Bonerandi JJ
Service de Dermatologie, Hopital Ste Marguerite, Marseille, France.
In order to establish whether or not here is an association between
cancer and intense growth of seborrheic keratosis, the so-called
Leser-Trelat sign, we conducted a case control study in which the number
and features of seborrheic keratosis in 82 patients with recent solid
tumours, were compared with 82 age- and sex-matched controls. Neither
numbers nor features of seborrheic keratosis differed significantly
in
patients and controls. Eruptive seborrheic keratosis was noted in only
one patient and one control. This study showed that solid malignancies
are not generally associated with an increase in the number or size
of
seborrheic keratosis lesions, thus suggesting that they are not
controlled by a hypothetical secretion of growth factors by tumours.
Our
results suggest that Leser-Trelat is either a coincidence, or at most
a
very rare sign of unusual types of cancer. We also showed that multiple
cherry angiomas, previously reported to be a paraneoplastic sign, are
not regularly associated with solid tumours.
===========================================================
39.) [Useful cutaneous markers of internal malignancy in the early
stage].
===========================================================
Gan To Kagaku Ryoho 1988 Apr;15(4 Pt 2-3):1564-8 Related Articles,
Books
Mori S
Dept. of Dermatology, Gifu University School of Medicine.
Numerous skin changes are correlated with internal malignancy. These
skin changes are collectively called dermadromes of internal malignancy
or syndroma dermato-tumorale. The skin markers of internal malignancy
can be classified into 1) skin metastasis, 2) paraneoplastic dermatoses,
3) cutaneous manifestations of the systemic carcinogenic disease process
and 4) cancer-malformation syndrome. For diagnosis of the early stage
of
internal malignancy, paraneoplastic dermatoses are the most important
among other skin changes. Above all, dermatomyositis, figurate
erythemas, erythroderma and a number of bullous dermatoses (e.g.,
bullous pemphigoid, pemphigus vulgaris and dermatitis herpetiformis,
Sweet' syndrome, pruritus, prurigo, acanthosis nigricans, Leser-Trelat
sign, alopecia mucinosa, acquired ichthyosis, Bazex' syndrome,
hypertrichosis aquisita lanuginosa) are among the paraneoplastic
dermatoses. A total of 405 cases of syndroma dermato-tumorale except
cases of skin metastasis were reported for recent 7 years (1980-1986)
only in the dermatological field in Japan. Among them, cases of
paraneoplastic dermatoses number 354 accounting for the majority.
Finally, brief consideration is given to the relationship between the
above mentioned skin manifestations and internal malignancy.
===========================================================
40.) [Gastrointestinal carcinoma with skin diseases from the standpoint
of surgery].
===========================================================
Gan To Kagaku Ryoho 1988 Apr;15(4 Pt 2-3):1560-3 Related Articles,
Books
Nishidoi H, Koga S, Kanbe N
1st Dept. of Surgery, Tottori University School of Medicine.
We encountered 21 patients with gastrointestinal carcinoma accompanied
with skin diseases such as acanthosis nigricans, dermatomyositis,
pemphigoid, erythrodermia, ichthyosis vulgaris, herpes zoster,
Leser-Trelat's sign, Recklinghausen's disease and Gardner's syndrome.
We
have discussed such cases from the standpoint of surgery. There were
16
cases (76%) with gastric carcinoma, which were almost in the far
advanced stage. Carcinomas of the other patients were seen in the
esophagus, liver, pancreas, small intestine and rectum. Although skin
lesions appeared before the onset of gastrointestinal symptoms in almost
all cases, detection of carcinomas was very difficult until the symptoms
emerged. In 6 of 21 patients (29%), carcinomas were detected by only
skin manifestation, and they proved to be gastric cancer in all cases.
Although the relationship of gastrointestinal carcinoma and skin
diseases was unclear, we presented a 70-year-old woman with acanthosis
nigricans accompanied with gastric cancer, whose skin manifestation
was
reduced by the therapy for gastric cancer. Therefore, some of these
skin
manifestation may be a symptom of the biological characteristics of
the
gastrointestinal carcinoma.
===========================================================
41.) [Leser-Trelat sign in adenocarcinoma of the sigmoid colon--a rare
clinical picture].
===========================================================
Z Hautkr 1987 Jun 1;62(11):875-6 Related Articles, Books
Hodak E, Halevy S, Ingber A, Engelstein D, Sandbank M
We report on a 75-year-old man showing the very rare association of
Leser-Trelat's sign and adenocarcinoma of the sigmoid colon. Our case
is
the second one reported so far.
===========================================================
42.) [Acanthosis nigricans maligna and Leser-Trelat sign in double
malignancy of the breast and stomach].
===========================================================
Z Hautkr 1987 Mar 1;62(5):344-66 Related Articles, Books
Stieler W, Plewig G
A female patient with primary cancer of the breast and the stomach
developed acanthosis nigricans maligna and Leser-Trelat's sign.
Acanthosis nigricans maligna is a well-known cutaneous marker of
internal malignancy. It may be intensified by radiotherapy. A variant
is
called florid cutaneous papillomatosis. Leser-Trelat's sign is a rare
cutaneous marker of internal neoplasms. According to the literature,
we
present 46 patients showing Leser-Trelat's sign. Neither Leser nor
Trelat described this sign.
===================================================================
43.) Beitrage Zur Fruhdiagnose des darmcarcinoms (Hereditasverhaltnisse
und Hautveranderungen)
hollander E
Dtsch Med Woschenschr 1900;26:483-5
===================================================================
===================================================================
DATA-MEDICOS/DERMAGIC-EXPRESS No 2-(92) 05/03/2.000 DR. JOSE
LAPENTA R.
===================================================================
|