| The Larva
Migrans Syndrome/ El sindrome de Larva Migrans.
Data-Medicos
Dermagic/Express No. 2-(89)
23 Febrero 2.000 23 February 2.000
~ El Sindrome Larva Migrans ~
~ The Larva Migrans Syndrome ~
EDITORIAL ESPANOL
=================
Hola amigos de al red, DERMAGIC de nuevo con ustedes. El tema de hoy
EL SINDROME DE LARVA MIGRANS Nos encantan las mascotas, sobre todo
los
perros y gatos. Pero en la mierda
de estos bellos animales hay unos parasitos que pueden pasar a la
pielcuando la tocamos o ingerimos, Mas aun algunos de estos parasitos
pueden MIGRAR hacia organos internos como cavidad visceral, ojo, cerebro
y otros. El sitio favorito para contraerla es la PLAYA donde nuestras
lindas mascotas hacen su mierda. Luego venimos nosotros e ingenuamente
la pisamos. Tambien en los hogares donde hay perros no controlados
por
el veterinario. En fin una enfermedad mas donde el hombre es
accidentalmente contaminado por el animal. En el caso de la LARVA
MIGRANS CUTANEA (SUPERFICIAL) quiza no represente grandes problemas,
pero en el caso de LA LARVA MIGRANS VISCERAL (PROFUNDA) la historia
es
OTRA. De modo pues que cuiden las lindas mascotas. Espero que disfruten
estas 67 referencias.
En el attach: la larva, el niño y la mascota.
Saludos a todos !!!
Dr. Jose Lapenta R.,,,
EDITORIAL ENGLISH
=================
Hello friends of to the net, DERMAGIC again with you. Today's topic
THE
LARVA MIGRANS SYNDROME. We love pets, mainly the dogs and cats.
But in
the fecal grounds of these beautiful animals there are some parasites
that can pass to the skin when we touch or eat it, But some of
these
parasites even can GO toward internal organs as visceral cavity, eye,
brain and others. The favorite place to contract it is the BEACH where
our pretty pets make its fecal grounds (shit). Then we come and frankly
we put our foot above them. Also in the homes where there are dogs
not
controlled by the veterinarian. In short an illness but where the man
is
accidentally polluted for the animal. In the case of the CUTANEOUS
LARVA
MIGRANS (SUPERFICIAL) doesn't maybe represent big problems, but in
the
case of THE VISCERAL LARVA MIGRANS (PROFUNDUS) the history is ANOTHER.
So that you have to take care of the pretty pets. I hope enjoy these
67
references.
In the attach: the larva, child and the pet
Greetings to ALL, !!
Dr. Jose Lapenta R.,,,
===================================================================
REFERENCIAS BIBLIOGRAFICAS / BIBLIOGRAPHICAL REFERENCES
===================================================================
============================================================
0.) CUTANEOS, VISCERAL and OCULAR LARVA MIGRANS
============================================================
1.) Souvenir from the Hamptons - a case of cutaneous larva migrans
of
six
months' duration.
2.) Effectiveness of a new therapeutic regimen with albendazole in
cutaneous larva migrans.
3.) [Migrant erythema as clinical presentation of cutaneous larva
migrans
in Mexico City]
4.) Larva migrans within scalp sebaceous gland.
5.) Cutaneous larva migrans, sacroileitis, and optic neuritis caused
by
an
unidentified organism acquired in Thailand.
6.) Perianal cutaneous larva migrans in a child.
7.) [Infections with Baylisascaris procyonis in humans and raccoons]
8.) Cutaneous larva migrans complicated by erythema multiforme [see
comments]
9.) Cutaneous larva migrans associated with water shoe use.
10.) Cutaneous larva migrans infection in the pediatric foot. A review
and
two case reports.
11.) Creeping eruption of larva migrans--a case report in a beach volley
athlete.
12.) Albendazole: a new therapeutic regimen in cutaneous larva migrans.
13.) A primary health care approach to an outbreak of cutaneous larva
migrans.
14.) Autochthonous cutaneous larva migrans in Germany.
15.) High prevalence of Ancylostoma spp. infection in dogs, associated
with
endemic focus of human cutaneous larva migrans, in Tacuarembo, Uruguay.
16.) Persistent cutaneous larva migrans due to Ancylostoma species.
17.) [A case of Dirofilaria repens migration in man]
18.) [Cutaneous larva migrans, autochthonous in France. Apropos of
a
case]
19.) Cutaneous larva migrans in travelers: synopsis of histories,
symptoms,
and treatment of 98 patients.
20.) [Nematode larva migrans. On two cases of filarial infection]
21.) Larva migrans that affect the mouth.
22.) Immunological studies on human larval toxocarosis.
23.) [Larva migrans]
24.) Effect of albendazole on Ancylostoma caninum larvae migrating
in
the
muscles of mice.
25.) [Ocular manifestations of toxocariasis]
26.) Toxocara infestations in humans: symptomatic course of toxocarosis
correlates significantly with levels of IgE/anti-IgE immune complexes.
27.) [Long-term observations of ocular toxocariasis in children and
youth]
28.) [A case of uveitis due to gnathostoma migration into the vitreous
cavity]
29.) [The ocular form of toxocariasis]
30.) [Visceral larval migrans (Human toxocariasis) cause of
hypereosinophilia and visceral granulomas in adults]
31.) Visceral larva migrans syndrome complicated by liver abscess.
32.) Visceral larva migrans and tropical pyomyositis: a case report.
33.) [2 cases of toxocariasis (visceral larva migrans)]
34.) [Visceral larva migrans. A rare cause of eosinophilia in adults]
35.) [Visceral larva migrans: a mixed form of presentation in an adult.
The
clinical and laboratory aspects]
36.) Visceral larva migrans induced eosinophilic cardiac pseudotumor:
a
cause of sudden death in a child.
37.) [Toxocariasis. A cosmopolitan parasitic zoonosis]
38.) Visceral larva migrans mimicking rheumatic diseases.
39.) Hepatic granulomas due to visceral larva migrans in adults:
appearance
on US and MRI.
40.) [Ascaridiasis zoonoses: visceral larva migrans syndromes]
41.) Hepatic visceral larva migrans: evolution of the lesion, diagnosis,
and role of high-dose albendazole therapy.
42.) Neuroimaging studies of cerebral "visceral larva migrans" syndrome.
43.)[Acute eosinophilic pneumonia and the larva migrans syndrome:
apropos
of a case in an adult]
44.)Toxocariasis simulating hepatic recurrence in a patient with Wilms'
tumor.
45.) Hepatic imaging studies on patients with visceral larva migrans
due
to
probable Ascaris suum infection.
46.) Encephalopathy caused by visceral larva migrans due to Ascaris
suum.
47.) [Imported skin diseases (see comments)]
48.) [Incidence of Toxocara ova--especially ova of visceral larva
migrans
in beach sand of Warnemunde in 1997]
49.) Pets and Parasites.
50.) Cutaneous larva migrans in travelers: synopsis of histories,
symptoms,
and treatment of 98 patients.
51.) Cutaneous larva migrans.
52.)[Current therapeutic possibilities in cutaneous larva migrans]
53.) Cutaneous larva migrans due to Pelodera strongyloides.
54.) Oral albendazole for the treatment of cutaneous larva migrans.
55.) Cutaneous larva migrans in northern climates. A souvenir of your
dream
vacation.
56.) Creeping eruption. A review of clinical presentation and management
of
60 cases presenting to a tropical disease unit.
57.) Dermatoses associated with travel to tropical countries: a
prospective
study of the diagnosis and management of 269 patients presenting to
a
tropical disease unit.
58.) Larva currens and systemic disease.
59.) Hookworm folliculitis.
60.) [Prurigo and further diagnostically significant skin symptoms
in
strongyloidosis]
61.) Gnathostomiasis, or larva migrans profundus.
62.) Visceral larva migrans caused by Trichuris vulpis.
63.) Creeping disease due to larva of spiruroid nematoda.
64.) Creeping eruption due to larvae of the suborder Spirurina--a newly
recognized causative parasite.
65.) Linear lichen planus mimicking creeping eruption.
66.) Diagnosis and management of Baylisascaris procyonis infection
in an
infant with nonfatal meningoencephalitis.
67.) [Human gnathostomiasis. The first evidence of the parasite in
South
America]
68.) Efficacy of ivermectin in the therapy of cutaneous larva migrans
[letter]
============================================================
============================================================
* CUTANEOUS LARVAL MIGRANS (Creeping Eruption) *
============================================================
SOURCE:
Mandell, Douglas and Bennett's
Principles and Practice of Infectious Diseases
Fourth Edition
Cutaneous larval migrans is characterized as serpiginous, reddened,
elevated, pruritic skin lesions usually caused by Ancylostoma
braziliense,
the dog and cat hookworm. 1,20 Other animal hookworms including A.
caninum,
Uncinaria stenocephala, Bunostomum phlebotomum, and others; the human
hookworms, Strongyloides stercoralis and Gnathostoma spinigerum; and,
rarely, insect larvae can cause similar findings. Like human hookworms,
A.
braziliense larvae infect dogs and cats by burrowing through the skin.
The
adults reside in the intestine and shed eggs, which undergo development
into infectious larvae outside the body in places protected from
desiccation and temperature extremes, such as sandy, shady areas around
beaches or under houses. Infections are most common in warmer climates
such
as the southeastern United States and occur in children more commonly
than
in adults. Larvae penetrate the skin, causing tingling followed by
itching,
vesicle formation, and typically raised, reddened, serpiginous tracks
that
mark the prior route of the parasite. In severe infections, persons
may
have hundreds of tracks. Little further development of the parasite
occurs.
Usually there are few, if any, systemic symptoms, but some reports
have
documented lung infiltrates and, rarely, severe lung dysfunction and
recovery of parasites in the sputum. Eosinophilia has been noted in
some
infections. The skin lesions are readily recognized, and the diagnosis
is
made clinically. Biopsy specimens usually show an eosinophilic
inflammatory
infiltrate, but the migrating parasite is usually not identified. For
this
reason, biopsies are usually not indicated to establish the diagnosis.
Without treatment, skin lesions gradually disappear. Both topical (10%
aqueous suspension qid) thiabendazole and oral administration
(25 mg/kg
bid for 2 days) are effective. In one study, most patients treated
with
thiabendazole responded within the first week compared to the more than
4
weeks required for comparable improvement in the placebo-treated group.
Successful treatment with albendazole or ivermectin has been
reported.
===========================================================
* VISCERAL LARVA MIGRANS (Toxocariasis) *
===========================================================
Visceral larva migrans (VLM) is a syndrome characterized in its most
florid
state by eosinophilia, fever, and hepatomegaly. It is caused primarily
by
infection with Toxocara canis but also be T. cati and other helminths
less
frequently.
----------------------
Life Cycle in the Dog
----------------------
Toxocara canis infects dogs and related mammals by a number of
mechanisms.
1 Most commonly, ingested eggs hatch in the small intestine, and the
resulting larvae migrate to the liver, lung, and trachea. They are
then
swallowed and mature in the lumen of the small intestine, where eggs
are
shed. Other larvae migrate to and remain dormant in the muscles but
are
capable of development even years after the primary infection,
particularly
in pregnant bitches. During pregnancy, larvae again develop and infect
the
pups transplacentally and transmammarily. Not uncommonly, infective
larvae
are found in the feces of the pups. Eggs are not infectious when passed
in
the feces and take 3–4 weeks to develop. They are hardy and often remain
viable for months. Large numbers of viable eggs contaminate the
environment
because of the high prevalence of infection in dogs and the ability
of
eggs
to survive relatively harsh environmental conditions.
Infection in Humans
-------------
Prevalence
------------
Toxocariasis is prevalent wherever dogs are found and Toxocara eggs
are
able to survive. The prevalence of infection or disease in humans is
not
known, but seroepidemiology studies show wide differences in prevalence
depending on the population tested. In the United States, seropositivity
ranged from 2.8 percent in an unselected population to 23.1 percent
in a
kindergarten population in the southern United States to 54 percent
in a
selected rural community. None of the seropositive persons had
recognizable
disease.
------------------------
Clinical Manifestations
-----------------------
VLM occurs most commonly in children less than 6 years of age. Disease
manifestations vary and range from asymptomatic infection to fulminant
disease and death, but it is increasingly appreciated that most
infections
are asymptomatic. Those who come to medical attention most commonly
complain of cough, fever, wheezing, and other generalized symptoms.
The
liver is the organ most frequently involved, and hepatomegaly is a
common
finding, although almost any organ can be affected. Splenomegaly occurs
in
a minority, and lymphadenopathy has been noted. Lung involvement with
radiologic findings has been documented in 32–44 percent, but
respiratory
distress occurs rarely. Skin lesions such as urticaria and nodules
have
also been described. Seizures have been noted to occur with increased
frequency in VLM, but severe neurologic involvement is infrequent.
Eye
involvement in VLM is unusual but has been documented (see below under
"Ocular Larva Migrans"). Eosinophilia, usually accompanied by
leukocytosis,
is the hallmark of VLM. Other laboratory findings include
hypergammaglobulinemia and elevated isohemagglutinin titers to A and
B
blood group antigens, which are due to the host's immune response to
cross-reacting antigens on the surface of T. canis larvae.
------------
Diagnosis
------------
The diagnosis of VLM is usually suggested clinically by the presence
of
eosinophilia and/or leukocytosis in a young child accompanied by
hepatomegaly or signs and symptoms of other organ involvement. A history
of
pica and exposure to puppies is common. Patients are more commonly
black
and from rural areas. The diagnosis is definitively confirmed by finding
larvae in the affected tissues by histologic examination or by digestion
of
tissue; however, larvae are frequently not found. The enzyme-linked
immunosorbent assay (ELISA) employing extracts or excretory-secretory
products of T. canis larvae appears specific and useful in confirming
the
clinical diagnosis. 8 However, toxocara antibody titers in populations
without clinically apparent VLM vary dramatically, and elevated titers
cannot definitively establish the diagnosis.
----------------------
Differential Diagnosis
----------------------
Eosinophilia, fever, and hepatomegaly are caused by other parasitic
infections. These include acute schistosomiasis, Fasciola hepatica
infections, Ascaris lumbricoides abscess of the liver, acute liver
fluke
infections (Clonorchis sinensis and Opisthorchis viverrini),
complications
from Echinococcus infection of the liver, Capillaria hepatica, and
other
invasive helminths. Diseases not caused by parasitic infections should
also
be considered. Children with mild disease may manifest only
eosinophilia.
-------------------------
Treatment and Management
-------------------------
Most patients recover without specific therapy. Treatment with
anti-inflammatory or anthelmintic drugs may be considered with severe
complications that are usually due to involvement of the brain, lungs,
or
heart. There is no proven effective therapy, although thiabendazole,
mebendazole, diethylcarbamazine, and other anthelmintics have been
used.
Indeed, injury to the parasite may provoke a more intense inflammatory
response leading to worsening of the clinical picture. Corticosteroids
have
been used with and without specific antilarval therapy, with some
reports
of improvement.
------------
Prevention
------------
VLM can be easily prevented by a number of simple but effective measures
that prevent T. canis eggs from contaminating the environment and
children
from ingesting eggs. Dogs, particularly puppies, should be periodically
tested and treated for T. canis and other worms. Pica should be
prevented.
===============================================
* Ocular Larva Migrans *
================================================
Ocular larval migrans (OLM) is caused by an infection of the eye with
T.
canis larvae. Although a present or past history of clinically
recognized
VLM has occasionally been noted, almost all patients present with
unilateral eye involvement without a past history or present systemic
symptoms or signs. Presumably, a larva by chance becomes entrapped
in
the
eye, resulting in an eosinophilic inflammatory mass. Children are most
commonly affected and, on the average, are older (mean, 8.6 years in
one
study) than those diagnosed with VLM. The findings are most commonly
those
of a posterior or peripheral inflammatory mass. In fact, this entity
was
first recognized after examination of eyes enucleated for the treatment
of
presumed retinoblastoma. Eosinophilia, hepatomegaly, and other
signs
and
sympoms of VLM are lacking. The diagnosis is established clinically.
Although the serum titers to toxocara larvae are higher than those
of a
control population, many patients with OLM have low or negative titers.
However, elevated vitreous 11 and aqueous fluid titers to toxocara
larvae
compared to serum levels have been documented and appear to be useful
in
establishing the diagnosis. There is no specific therapy.
============================================================
============================================================
1.) Souvenir from the Hamptons - a case of cutaneous larva migrans
of
six
months' duration.
============================================================
Mt Sinai J Med 1999 Oct-Nov;66(5-6):334-5 (ISSN: 0027-2507)
Esser AC; Kantor I; Sapadin AN [Find other articles with these Authors]
Department of Dermatology, Mount Sinai School of Medicine, One East
100th
Street New York, NY, USA.
Cutaneous larva migrans is a distinctive serpiginous eruption caused
by
a
reaction to burrowing hookworms. The infection is usually self-limited,
normally lasting 2-8 weeks, but may persist for more than a year if
misdiagnosed. Biopsies of the creeping eruption rarely reveal an
organism.
Thus, it is important for the infection to be recognized clinically,
so
that effective treatment may begin. We found topical thiabendazole
to be
fast and effective in treating this case of cutaneous larva migrans
of
six
months' duration.
============================================================
2.) Effectiveness of a new therapeutic regimen with albendazole in
cutaneous larva migrans.
============================================================
Eur J Dermatol 1999 Jul-Aug;9(5):352-3 (ISSN: 1167-1122)
Veraldi S; Rizzitelli G [Find other articles with these Authors]
Institute of Dermatological Sciences, IRCCS, University of Milan, Via
Pace
9, 20122 Milan, Italy.
Twenty-four (13 males and 11 females) adult Caucasian patients affected
by
cutaneous larva migrans, characterized by extensive and/or multiple
lesions, were treated with oral albendazole according to a new
therapeutic
regimen (400 mg/day for 7 days). No other topical or systemic drug
was
used
nor any physical treatment. All patients were cured at the end of the
therapy. No recurrence was observed. No side effect was either
complained
of or observed, nor was any laboratory abnormality recorded. On the
basis
of this study, albendazole is effective in cutaneous larva migrans
characterized by extensive and/or multiple lesions. This new therapeutic
regimen avoids no response and recurrence, which are not uncommonly
observed following shorter (e.g.: 1-5 days) therapies with albendazole.
The
longer duration of the therapy is not accompanied by the appearance
of
more
severe and/or new side effects or laboratory abnormalities.
============================================================
3.) [Migrant erythema as clinical presentation of cutaneous larva
migrans
in Mexico City]
[Eritema migratorio como presentacion clinica de larva migrans cutanea
en
la ciudad de Mexico.]
============================================================
Gac Med Mex 1999 May-Jun;135(3):235-8 (ISSN: 0016-3813)
Halabe-Cherem J; Nellen-Hummel H; Jaime-Gamiz I; Lifshitz-Guinzberg
A;
Morales-Cervantes R; Gallegos-Hernandez V; Malagon-Rangel J [Find other
articles with these Authors]
Cutaneous larva migrans (CLM) is a ubiquitous self-limited skin
eruption,
most frequently caused by the larvae of dog and cat hookworms. Although
CLM
is most frequent in tropical climates, the infection is becoming more
common in urban areas. CLM has been frequently misdiagnosed and/or
treated
inappropriately, and mimics rheumatic, infectious, vascular, or
dermatologic diseases. We here in report the clinical presentation
and
management of 18 cases of CLM.
============================================================
4.) Larva migrans within scalp sebaceous gland.
============================================================
Rev Soc Bras Med Trop 1999 Mar-Apr;32(2):187-9 (ISSN: 0037-8682)
Guimaraes LC; Silva JH; Saad K; Lopes ER; Meneses AC [Find other
articles
with these Authors]
Faculdade de Medicina do Triangulo Mineiro, Hospital Helio Angotti
(Associacao de Combate ao Cancer do Brasil Central), Universidade de
Uberaba, MG.
A case of larva migrans or serpiginous linear dermatitis on the scalp
of
a
teenager is reported. An ancylostomid larva was found within a sebaceous
gland acinus. The unusual skin site for larva migrans as well as the
penetration through the sebaceous gland are highlighted. The probable
mechanism by which the parasite reached the skin adnexa is discussed.
============================================================
5.) Cutaneous larva migrans, sacroileitis, and optic neuritis caused
by
an
unidentified organism acquired in Thailand.
============================================================
J Travel Med 1998 Dec;5(4):223-5 (ISSN: 1195-1982)
Potasman I; Feiner M; Arad E; Friedman Z [Find other articles with these
Authors]
Infectious Diseases Unit, and Ophthalmology Department, Bnai Zion
Medical
Center, the Rappaport School of Medicine, Technion, Haifa, Israel.
We report the case of a 32-year-old pregnant woman with an unidentified
intraocular parasite. The parasite, which had been acquired in Thailand,
caused cutaneous larva migrans, sacroileitis, and 2 years later optic
neuritis and panuveitis. The patient was successfully treated with
ivermectin and albendazole. The diagnostic possibilities of this
peculiar
presentation are discussed. Parasitic infections are a leading cause
of
medical problems in travelers to tropical countries.1 While most
parasites
cause gastrointestinal problems, some may migrate throughout the body
and
lodge in critical organs. Ocular parasitic infections may occur by
direct
inoculation onto the eye,2 or incidentally during systemic migration.
Subconjunctival parasites are easily diagnosed by removal and careful
microscopic examination.3 Parasites, which lodge within the eye, are
more
difficult to diagnose, especially if not removed. In this report we
describe a patient who presented with an intraocular parasite causing
optic
neuritis and panuveitis, 2 years after travel to Thailand.
============================================================
6.) Perianal cutaneous larva migrans in a child.
============================================================
Pediatr Dermatol 1998 Sep-Oct;15(5):367-9 (ISSN: 0736-8046)
Grassi A; Angelo C; Grosso MG; Paradisi M [Find other articles with
these
Authors]
Department of Pediatric Dermatology, Istituto Dermopatico
dell'Immacolata,
Rome, Italy.
Cutaneous larva migrans (CLM) is a dermatosis characterized by the
presence
of parasites which migrate into the skin, forming linear or serpiginous
lesions. We report a child with cutaneous larva migrans of interest
because
of the involvement of an unusual site and the patient's age. We confirm
the
efficacy of therapy consisting of administration of albendazole by
mouth.
============================================================
7.) [Infections with Baylisascaris procyonis in humans and raccoons]
[Infecties met Baylisascaris procyonis bij de mens en de wasbeer.]
============================================================
Tijdschr Diergeneeskd 1998 Aug 15;123(16):471-3 (ISSN:
0040-7453)
Zagers JJ; Boersema JH [Find other articles with these Authors]
Afdeling Parasitologie en Tropische Diergeneeskunde, Hoofdafdeling
infectieziekten en Immunologie, Faculteit der Diergeneeskunde,
Universiteit
Utrecht.
Baylisascaris procyonis is an ascarid which parasitizes the small
intestine
of raccoons. The parasite is not very pathogenic in the raccoon because
larvae do not migrate in this host. In other animals the larvae migrate
through the body. They do not develop into adult worms in the intestine
but
rather become encysted in granulomas, showing a preference for the
brain.
In humans these larvae cause different larva migrans syndromes. Patients
with neural larva migrans syndrome show severe brain symptoms and the
disease is sometimes fatal. This article describes the life cycle of
the
worm and the incidence, symptoms, diagnosis, treatment, and prevention
of
larva migrans syndromes, paying special attention to the Dutch
situation.
============================================================
8.) Cutaneous larva migrans complicated by erythema multiforme [see
comments]
============================================================
Cutis 1998 Jul;62(1):33-5 (ISSN: 0011-4162)
Vaughan TK; English JC 3rd [Find other articles with these Authors]
Dermatology Service, Evans Army Community Hospital, Fort Carson,
Colorado,
USA.
Cutaneous larva migrans is an intensely pruritic serpiginous eruption
caused by the dog or cat hookworm. Often, the disease is self-limiting
and
no other significant pathology develops; however, a significant
localized
inflammatory response to the nematode is extremely common. We present
a
case of cutaneous larva migrans in which a systemic inflammatory process
ensued that was characteristic of erythema multiforme. We discuss
possible
mechanisms of this complication and review the literature.
============================================================
9.) Cutaneous larva migrans associated with water shoe use.
============================================================
J Eur Acad Dermatol Venereol 1998 May;10(3):271-3 (ISSN:
0926-9959)
Swanson JR; Melton JL [Find other articles with these Authors]
Division of Dermatology, Loyola University Medical Center, Maywood,
IL
60153, USA.
It has been long suspected that footwear is protective against cutaneous
larva migrans. This case report describes a woman who developed
cutaneous
larva migrans despite wearing 'protective' footwear. We forward a
hypothesis by which recently popular water shoes may actually be
conducive
to the development of cutaneous larva migrans rather than having a
protective function.
============================================================
10.) Cutaneous larva migrans infection in the pediatric foot. A review
and
two case reports.
============================================================
J Am Podiatr Med Assoc 1998 May;88(5):228-31 (ISSN: 8750-7315)
Mattone-Volpe F [Find other articles with this Author]
Children's Hospital of Philadelphia, PA, USA.
Cutaneous larva migrans is the result of infestation of human skin by
helminth larvae, which burrow through the epidermis. This route of
infestation makes the foot a typical site for origination of this
infection. Children, who frequently play barefoot in locations where
the
most common of the helminth larvae, the dog and cat hookworms, are
endemic,
are at particular risk for this disorder. This article reviews the
differential diagnosis of cutaneous larva migrans and current concepts
in
management. Two cases of related children who presented to their
pediatricians with this condition are reported.
============================================================
11.) Creeping eruption of larva migrans--a case report in a beach volley
athlete.
============================================================
Int J Sports Med 1997 Nov;18(8):612-3 (ISSN: 0172-4622)
Biolcati G; Alabiso A [Find other articles with these Authors]
S. Gallicano Institute, Institute of Sports Sciences, Rome, Italy.
The authors describe a case of cutaneous larva migrans in a beach volley
athlete. This pathology is found more often in tropical zones than in
European countries. There are no previous publications with regard
to
this
condition in athletes. The nematode responsible for this affliction
often
is the Ancylostoma braziliense. Larval stage of the nematode migrates
through the skin; within 72 hours after larval penetration, serpiginous,
elevated tunnels are observed. This affliction can be complicated by
Loeffler's syndrome. In the case described only dermatological
involvement
was observed. The patient was treated with 400 mg albendazole tablets
twice
a day for five days. Within two days of therapy the patient reported
less
itching; a medical control after ten days did not reveal any signs
of
active infection.
============================================================
12.) Albendazole: a new therapeutic regimen in cutaneous larva migrans.
============================================================
Int J Dermatol 1997 Sep;36(9):700-3 (ISSN: 0011-9059)
Rizzitelli G; Scarabelli G; Veraldi S [Find other articles with these
Authors]
Institute of Dermatological Sciences, IRCCS, University of Milan, Italy.
BACKGROUND: Various therapeutic modalities have been used to treat
cutaneous larva migrans, including physical treatments (cryotherapy),
topical drugs (tiabendazole), and systemic drugs (tiabendazole,
albendazole, and ivermectin). Physical treatments are often ineffective
and
not devoid of side-effects. Topical tiabendazole is difficult to find
in
many countries; it is effective orally but frequently causes
side-effects.
Ivermectin has been used in a small number of patients. METHODS: Eleven
(six men and five women) adult patients with cutaneous larva migrans
characterized by multiple and/or diffuse lesions were treated with
oral
albendazole (400 mg daily for 7 days). No other topical or systemic
drugs
were used and no physical treatment was given. RESULTS: All patients
were
cured at the end of treatment. No side-effects were complained of or
observed, and no laboratory abnormalities were recorded. No recurrences
were observed. CONCLUSIONS: Albendazole is effective in the treatment
of
cutaneous larva migrans characterized by multiple and/or diffuse
lesions.
This new therapeutic regimen can reduce the number of no responses
and
recurrences, sometimes observed following shorter (e.g. 3-5 days)
treatments with albendazole. The longer duration of treatment is not
accompanied by the appearance of new and/or more severe side-effects.
============================================================
13.) A primary health care approach to an outbreak of cutaneous larva
migrans.
============================================================
J S Afr Vet Assoc 1996 Sep;67(3):133-6 (ISSN: 0301-0732)
McCrindle CM; Hay IT; Kirkpatrick RD; Odendaal JS; Calitz EM [Find other
articles with these Authors]
Department of Production Animal Medicine, Faculty of Veterinary Science,
Medical University of Southern Africa, Medunsa, South Africa.
Primary health care (PHC) has been defined by the World Health
Organisation
as essential health care made universally accessible to community
members,
with their full participation, at a cost affordable to the community.
PHC
could therefore be used in the prevention and treatment of zoonotic
diseases in humans, as such diseases are more prevalent in disadvantaged
communities. The successful use of PHC principles in the treatment and
control of cutaneous larva migrans in children in a semi-rural,
low-income
community is discussed in this paper. Constraints to implementation
of
PHC
principles were identified as resistance from health care professionals,
lack of interdepartmental cooperation and bureaucratic delays. It is
concluded that PHC principles can be used successfully for the
prevention
and treatment of specific zoonoses provided that an aetiological
diagnosis
is made and the epidemiology of the condition understood. The results
also
confirmed the relevance of the veterinarian in the control of zoonotic
diseases as part of the PHC team.
============================================================
14.) Autochthonous cutaneous larva migrans in Germany.
============================================================
Trop Med Int Health 1996 Aug;1(4):503-4 (ISSN: 1360-2276)
Klose C; Mravak S; Geb M; Bienzle U; Meyer CG [Find other articles with
these Authors]
Institute for Tropical Medicine, Berlin, Germany.
Cutaneous larva migrans syndrome is extremely rare in Germany. However,
three cases of this syndrome were diagnosed in patients from Berlin,
Germany, in the summer of 1994. Exposure to the infective agent in
endemic
areas and close contact with animals were excluded. It is assumed that
the
extreme temperatures in summer 1994 favoured the conditions of
infection.
============================================================
15.) High prevalence of Ancylostoma spp. infection in dogs, associated
with
endemic focus of human cutaneous larva migrans, in Tacuarembo, Uruguay.
============================================================
Parasite 1996 Jun;3(2):131-4 (ISSN: 1252-607X)
Malgor R; Oku Y; Gallardo R; Yarzabal I [Find other articles with these
Authors]
Unidad de Biologia Parasitaria, Universidad de la Republica Oriental
del
Uruguay, Montevideo, Uruguay.
A helminthological survey of the intestinal parasites in stray dogs
was
conducted in urban and suburban area of Tacuarembo, Uruguay, during
winter
time. Eighty stray dogs captured in the city were necropsied. Seventy
nine
dogs (98.8%) were positive for helminth infection. Seventy seven (96.3%)
were parasitized by hookworms. Two species of hookworms were found:
Ancylostoma caninum 96.3% and A. braziliense 49.4%. This is the first
report of the prevalence of A. braziliense in Uruguay. Considering
that
incidences of human cutaneous larva migrans caused by the migration
of
hookworms larvae were restricted mainly to the northern part of Uruguay
and
that only A. caninum were reported to be prevalent in the southern
part,
it
is supposed that A. braziliense is the primary causative agent of human
cutaneous larva migrans in Uruguay.
============================================================
16.) Persistent cutaneous larva migrans due to Ancylostoma species.
============================================================
South Med J 1996 Jun;89(6):609-11 (ISSN: 0038-4348)
Richey TK; Gentry RH; Fitzpatrick JE; Morgan AM [Find other articles
with
these Authors]
Dermatology Service, Department of Medicine, Fitzsimons Army Medical
Center, Aurora, CO 80045, USA.
Cutaneous larva migrans is considered to be a self-limited parasitic
infection of about 2 to 8 weeks' duration, though it has been reported
to
persist for as long as 55 weeks. In this case, a healthy 47-year-old
white
man had multiple serpiginous lesions typical of cutaneous larva migrans
for
18 months. A biopsy taken 2 months before presentation showed a parasite
consistent with Ancylostoma species deep in a hair follicle. The patient
initially responded to topical thiabendazole, but relapse occurred when
therapy was discontinued. Oral thiabendazole cured the problem after
22
months of infestation. Cutaneous larva migrans may sometimes be
long-standing, here almost 2 years, even in a healthy patient. Organisms
may reside deep in the hair follicles. Topical thiabendazole may not
penetrate to this depth, necessitating oral thiabendazole therapy.
============================================================
17.) [A case of Dirofilaria repens migration in man]
[Sluchai migratsii Dirofilaria repens u cheloveka.]
============================================================
Med Parazitol (Mosk) 1996 Jan-Mar;(1):44 (ISSN: 0025-8326)
Artamonova AA; Nagornyi SA [Find other articles with these Authors]
The paper reports a case of Dirofilaria repens subcutaneous parasitism
with
the larva migrans phenomenon in the North Causasus area where
epidemiological prerequisites are available for spread of
dirofilariasis.
The clinical picture, surgical intervention, and the diagnosis of the
infection are presented. The parasite is defined by the authors as
Dirofilaria repens.
============================================================
18.) [Cutaneous larva migrans, autochthonous in France. Apropos of
a
case]
[Larva migrans cutanee autochtone en France. A propos d'un cas.]
============================================================
Ann Dermatol Venereol 1995;122(10):711-4 (ISSN: 0151-9638)
Zimmermann R; Combemale P; Piens MA; Dupin M; Le Coz C [Find other
articles
with these Authors]
Clinique de Dermatologie, Hopital d'Instruction des Armees Desgenettes,
Lyon.
INTRODUCTION: Cutaneous larva migrans is rarely contracted in temperate
countries. CASE REPORT: When his house became flooded, he had to stand
for
a long period of time with mud up to the thigh. Some days later, he
developed multiple erythematous, serpiginous pruritic tracts moving
1-2
cm
per day over preexisting lesions of the right leg. Local and systemic
treatment with thiabendazole led to rapid and definitive cure.
DISCUSSION:
Cutaneous larva migrans results from the migration of hookworm larvae
in
the dead-end human host. It is mainly an imported disease and native
cases
in Europe as reported here are rare. This case demonstrates that the
conditions leading to the development of cutaneous larva migrans are
rarely
found simultaneously in temperate zones.
============================================================
19.) Cutaneous larva migrans in travelers: synopsis of histories,
symptoms,
and treatment of 98 patients.
============================================================
Clin Infect Dis 1994 Dec;19(6):1062-6 (ISSN: 1058-4838)
Jelinek T; Maiwald H; Nothdurft HD; Loscher T [Find other articles with
these Authors]
Department of Infectious Diseases and Tropical Medicine, University
Hospital, University of Munich, Germany.
The symptoms, medical history, and treatment of 98 patients with
cutaneous
larva migrans (creeping eruption) who attended a travel-related-disease
clinic during a period of 4 years are reviewed. This condition is caused
by
skin-penetrating larvae of nematodes, mainly of the hookworm Ancylostoma
braziliense and other nematodes of the family Ancylostomidae. Despite
the
ubiquitous distribution of these nematodes, in the investigated group
only
travelers to tropical and subtropical countries were affected; 28.9%
of
the
patients had symptoms for > 1 month, and for 24.5% the probable
incubation
period was > 2 weeks. The efflorescences typically were on the lower
extremities (73.4% of all locations). The buttocks and anogenital region
were affected in 12.6% of all locations, and the trunk and upper
extremities each were affected in 7.1%. Only a minority of patients
presented with eosinophilia or an elevated serum level of IgE. No other
laboratory data appeared to be related to the disease. Therapy with
topical
thiabendazole was successful for 98% of the patients. Systemic
antihelmintic therapy was necessary in two cases because of
disseminated,
extensive infection.
============================================================
20.) [Nematode larva migrans. On two cases of filarial infection]
[Wandernde Nematodenlarven. Uber zwei Falle von Filarienbefall.]
============================================================
Pathologe 1994 Jun;15(3):171-5 (ISSN: 0172-8113)
Bittinger A; Barth P; Kohler HH [Find other articles with these Authors]
Medizinisches Zentrum fur Pathologie der Philipps-Universitat Marburg.
With rapid air travel, so-called parasitic infections are becoming more
important in northern hemisphere and temperate climates. Parasitic
disease
is usually taken to imply infections caused by protozoa and helminths.
The
most important helminthic infections in man and with world-wide
incidence
are schistosomiasis, hookworm, and filariasis. We report the
clinico-pathological findings of two patients with filarial infection
of
soft tissue and lymphatic nodes.
============================================================
21.) Larva migrans that affect the mouth.
============================================================
Oral Surg Oral Med Oral Pathol 1994 Apr;77(4):362-7 (ISSN:
0030-4220)
Lopes MA; Zaia AA; de Almeida OP; Scully C [Find other articles with
these
Authors]
Faculty of Odontology, University of Campinas, Sao Paulo, Brazil.
As air travel expands, tropical diseases are increasingly likely to
be
encountered. We report a case of a nematode infection from dogs and
cats
that appeared in the mouth as larva migrans, and we review the
literature.
============================================================
22.) Immunological studies on human larval toxocarosis.
============================================================
Cent Eur J Public Health 1996 Dec;4(4):242-5 (ISSN: 1210-7778)
Uhlikova M; Hubner J; Kolarova L; Polackova M [Find other articles with
these Authors]
Postgraduate Medical School, Prague, Czech Republic.
The aim of the study was to characterize the antiparasite humoral
response
in patients with the syndrome of visceral larval toxocarosis. Specific
IgG,
specific IgE and total IgE immunoglobulins against Toxocara canis
excretory/secretory antigens (TES) were detected by using ELISA
technique.
Antibody response was studied in complete sera as well as in
immunoglobulin
fractions (IgG and IgE), isolation of which was performed on Protein
A
Sepharose. It was observed that removal of IgG from the serum samples
resulted mostly in increasing levels of anti-Toxocara IgE antibodies
what
agrees with the theory of the blocking effect of IgG in the immune
response. The results demonstrated a little correlation between slgG
and
slgE in the sera of symptomatic patients, examined in ELISA reaction.
============================================================
23.) [Larva migrans]
[Le larbish.]
============================================================
Sante 1995 Nov-Dec;5(6):341-5 (ISSN: 1157-5999)
Chabasse D; Le Clec'h C; de Gentile L; Verret JL [Find other articles
with
these Authors]
Laboratoire de parasitologie-mycologie, Consultations des maladies
parasitaires et tropicales, CHU, Angers, France.
Larbish, cutaneous larva migrans or creeping eruption, is a serpiginous
cutaneous eruption caused by skin penetration of infective larva from
various animal nematodes. Hookworms (Ancylostoma brasiliense, A.
caninum)
are the most common causative parasites. They live in the intestines
of
dogs and cats where their ova are deposited in the animal feces. In
sandy
and shady soil, when temperature and moisture are elevated, the ova
hatch
and mature into infective larva. Infection occurs when humans have
contact
with the infected soil. Infective larva penetrate the exposed skin
of
the
body, commonly around the feet, hands and buttocks. In humans, the
larva
are not able to complete their natural cycle and remain trapped in the
upper dermis of the skin. The disease is widespread in tropical or
subtropical regions, especially along the coast on sandy beaches. The
diagnosis is easy for the patient who is returning from a tropical
or
subtropical climate and gives a history of beach exposure. The
characteristic skin lesion is a fissure or erythematous cord which
is
displaced a few millimeters each day in a serpiginous track. Scabies,
the
larva currens syndrome due to Strongyloides stercoralis, must be
distinguished from other creeping eruptions and subcutaneous swelling
lesions caused by other nematodes or myiasis. Medical treatments are
justified because it shortens the duration of the natural evolution
of
the
disease. Topical tiabendazole is safe for localized invasions, but
prolonged treatment may be necessary. Oral thiabendazole treatment
for
three days is effective, but sometimes is associated with adverse
effects.
Trials using albendazole for one or four consecutive days appear more
efficacious. More recent trials using ivermectine showed that a single
oral
dose can cure 100% of the patients; thus, this drug looks very promising
as
a new form of therapy. Individual prophylaxis consists of avoiding
skin
contact with soil which has been contaminated with dog or cat feces.
Keeping dogs and cats off the beaches is illusory in tropical countries.
============================================================
24.) Effect of albendazole on Ancylostoma caninum larvae migrating
in
the
muscles of mice.
============================================================
Chung Kuo Chi Sheng Chung Hsueh Yu Chi Sheng Chung Ping Tsa Chih
12;3(214-7Unknown Paragraph TypeS1000-7423Unknown Paragraph Type
Xiao S; Ren H; You J; Zhao L; Li B; Zhang C [Find other articles with
these
Authors]
Institute of Parasitic Diseases, Chinese Academy of Preventive Medicine
(WHO Collaborating Centre for Malaria, Schistosomiasis and Filariasis),
Shanghai.
When mice inoculated with 1,000 third-stage larvae of Ancylostoma
caninum
for 1 week were treated intragastrically (ig) with albendazole (Alb)
75,
150 or 300 mg/kg.d for 3 days, the mean larva numbers collected from
the
muscles of each group were 2.7 +/- 1.7, 2.0 +/- 1.5 and 1.0 +/- 1.0,
respectively, being much less than that 205 +/- 68 of the control group.
In
mice treated ig with Alb 150 mg/kg.d for 3 days, the concentrations
of
Alb
and its effective metabolite, albendazole sulfoxide (AlbSO), were
determined in plasma and the muscles at different intervals after the
last
medication using high performance liquid chromatography. The results
showed
that only low concentrations of Alb were detected in both plasma and
the
muscles. However, higher concentrations of AlbSO were found not only
in
the
plasma (5.4-10.5 micrograms/ml), but also in the muscles (2.2-4.6
micrograms/g). The higher contents of AlbSO in the muscles would be
helpful
for killing the Ancylostoma larvae migrating in the muscles of mice.
============================================================
25.) [Ocular manifestations of toxocariasis]
============================================================
[Ocne prejavy toxokarozy.]
Bratisl Lek Listy 1999 Mar;100(3):161-3 (ISSN: 0006-9248)
Gerinec A; Slivkova D [Find other articles with these Authors]
Pediatric Ophthalmology Dpt, Faculty of Medicine, Comenius University,
Bratislava, Slovakia.
The paper reports about the ocular symptomatology of toxocariasis that
represents a severe parasitic disease especially in children. Recently,
the
incidence of this disease is increasing. Diagnostic process has improved
by
means of newly developed laboratory methods. Ocular findings on retina
are
in toxocariasis identified very late. Despite many antihelmintics,
steroids
and surgical treatment, a poor treatment success has been achieved,
and
the
sight remains often permanently severely affected. Because of the risk
of
blindness the most efficient arrangement is prophylaxy from the side
of
parents, teachers, veterinarions and the society as a whole. (Fig.
3,
Ref.
6.).
============================================================
26.) Toxocara infestations in humans: symptomatic course of toxocarosis
correlates significantly with levels of IgE/anti-IgE immune complexes.
============================================================
Parasite Immunol 1998 Jul;20(7):311-7 (ISSN: 0141-9838)
Obwaller A; Jensen-Jarolim E; Auer H; Huber A; Kraft D; Aspock H [Find
other articles with these Authors]
Department of Medical Parasitology, University of Vienna, Austria.
Infestations of humans with the parasitic nematode T. canis are common
in
both developing and industrialized countries. Most infestations induce
a
clinically inapparent course of infection, however, severe clinical
manifestations, i.e. visceral larva migrans (VLM) or ocular larva
migrans
(OLM) syndromes are observed. To find an explanation for the different
courses of toxocarosis we examined several serological parameters:
the
expression of (i) specific IgE (Immunoblot, IB), (ii) specific IgG
subclasses (IgG1-4, ELISA and the formation of (iii) IgE/anti-IgE immune
complexes. Serum samples were obtained from persons with symptomatic
(VLM,
OLM) and asymptomatic course (AS) of the infestation. As antigen, T.
canis
excretory/secretory (TES) antigen from L3 larvae was used. Reactivity
of
IgE against SDS-PAGE separated TES antigens was marginally higher in
toxocarosis patients (35%) than in asymptomatics (24%), but without
statistical significance. TES-specific IgG (1-4), predominant subclass
in
all three groups was IgG1, followed by IgG2, IgG4 and IgG3. Subclass
IgG1,
2, 4 showed significant differences between patients with VLM associated
symptoms and asymptomatic persons (P < 0.001) but not between patients
with
OLM associated symptoms and asymptomatics. Significantly elevated levels
of
IgE/anti-IgE immune complexes were detected in sera of patients with
symptomatic course of the disease, both VLM and OLM (P < 0.001).
Whereas
specific IgG may act via antibody dependent cell-mediated cytotoxicity
mechanisms, IgE/anti-IgE immune complexes might possibly participate
in
VLM
and OLM by inducing type III hypersensitivity.
============================================================
27.) [Long-term observations of ocular toxocariasis in children and
youth]
[Odlegle obserwacje toksokarozy ocznej u dzieci i mlodziezy.]
============================================================
Klin Oczna 1996;98(6):445-8 (ISSN: 0023-2157)
Krukar-Baster K; Zygulska-Mach H; Sajak-Hydzik K; Kubicka-Trzaska A;
Dymon
M [Find other articles with these Authors]
Katedry I Kliniki Okulistyki Collegium Medicum UJ w Krakowie.
PURPOSE: To evaluate the clinical status and ELISA test changes in a
group
of children with ocular toxocariasis. METHODS: We enrolled 37 patients
in
the studies. The follow-up period lasted at least 3 years (3-15 years)
after the diagnosis had been established. In all cases a complete
ophthalmological examination and actual ELISA test were performed.
We
compared the clinical status in two groups of patients: one with
positive
and the other with negative ELISA test at the time of control
examination.
RESULTS: In a majority of initially positive serological patients the
control ELISA test for Toxocara canis antigen was negative. In these
cases
various post-inflammatory lesions in the anterior and posterior pole
of
the
eye were present. In 8 cases the ELISA test was positive, despite the
absence of active inflammatory process. In 5 serologically positive
patients the active inflammation was observed. In more than 50% of
cases
the visual acuity was decreased. CONCLUSION: Ocular toxocariasis is
a
long-lasting, severe type of uveitis that requires long treatment and
causes dramatic visual impairment. ELISA test is a sensitive method
indicating the intensity of inflammation in ocular toxocariasis.
============================================================
28.) [A case of uveitis due to gnathostoma migration into the vitreous
cavity]
============================================================
Nippon Ganka Gakkai Zasshi 1994 Nov;98(11):1136-40 (ISSN:
0029-0203)
Sasano K; Ando F; Nagasaka T; Kidokoro T; Kawamoto F [Find other
articles
with these Authors]
Department of Ophthalmology, Nagoya National Hospital, Japan.
We report a 26 year-old male patient who had floaters and hyperemia
in
his
left eye following uveitis due to gnathostoma that had migrated into
the
vitreous cavity. Severe iridocyclitis and mild opacity of the vitreous
body
were observed, together with whitish-yellow subretinal tracks
accompanied
by dot and blot hemorrhages in the fundus. Slit lamp microscopic
examination revealed a worm which writhed in the vitreous cavity. We
performed vitrectomy to remove the worm from the anterior vitreous
uneventfully, followed by prompt subsidence of the inflammatory signs.
The
worm was identified as a third instar larva of Gnathostoma doloresi.
Eosinophilia and creeping eruption did not appear throughout the
follow-up
period. The patient was accustomed to eat live roaches and whitebait,
as
well as sliced raw beef liver.
============================================================
29.) [The ocular form of toxocariasis]
[Ocni forma larvalni toxokarozy.]
============================================================
Cesk Oftalmol 1994 Jun;50(3):186-90 (ISSN: 0009-059X)
Lobovska A; Zackova M [Find other articles with these Authors]
III. klinika infekcnich a tropickych nemoci 1. LF UK, Praha.
Ocular toxocariasis (ocular form of larval toxocariasis) arises mainly
unilaterally and represents no rare disease. On 3rd Department of
Infectology, 1st Faculty of Medicine, Charles University, Prague, 102
patients with proved larval toxocariasis were treated from 1981 to
1990.
Ocular toxocariasis concerned only one third of this number. Most
frequent
form was the retinal toxocaral granuloma (in 55.2%), positioned by
two
thirds at the posterior pole of retina. In one case, endophthalmitis
led
to
amaurosis of the eye. Clinical forms typical for ocular toxocariasis
are
presented. No statistically significant difference was observed in
treatment effects using thiobendazole or diethylcarbamazine. All
patients
with ocular toxocariasis were treated with systematic steroids.
============================================================
30.) [Visceral larval migrans (Human toxocariasis) cause of
hypereosinophilia and visceral granulomas in adults]
[Larva migrante visceral (toxocariasis humana) causa de hipereosinofilia
y
granulomas viscerales en el adulto.]
============================================================
Bol Chil Parasitol 1999 Jan-Jun;54(1-2):21-4 (ISSN: 0365-9402)
Sapunar J; Fardella P [Find other articles with these Authors]
Departamento de Medicina, Hospital Clinico, Universidad de Chile.
A 24-year-old woman 2-3 months after a normal parturation presented
geophagy. Due to hypermenorrhea she consulted a gynecologist and in
a
hemogram a 57% (6,893 x mm3) hypereosinophilia was detected. A chest
TAC
showed bilateral pulmonary nodules. The following tests resulted
positive:
ELISA IgG for toxocariasis 1:1000, isohemagglutinins anti A 1:2048
and
anti
B 1:512. The patient was treated with albendazole and prednisone during
10
days. One month after treatment eosinophilia decreased to 2.590 x mm3
and
ELISA IgG for toxocariasis descended to 1:128. Different aspects of
human
toxocariasis are commented. When hypereosinophia is observed in adult
patients, toxocariasis must be checked.
============================================================
31.) Visceral larva migrans syndrome complicated by liver abscess.
============================================================
Scand J Infect Dis 1999;31(3):324-5 (ISSN: 0036-5548)
Rayes A; Teixeira D; Nobre V; Serufo JC; Goncalves R; Valadares L;
Lambertucci JR [Find other articles with these Authors]
Department of Internal Medicine, Infectious Disease Branch, School
of
Medicine, Federal University of Minas Gerais, Belo Horizonte, Brazil.
We describe a case of visceral larva migrans syndrome complicated by
liver
abscess, pericardial effusion and ascites. To our knowledge, these
findings
have not been reported previously. The structural and immunological
alterations caused by visceral larva migrans are thought to lead to
the
development of visceral abscesses.
============================================================
32.) Visceral larva migrans and tropical pyomyositis: a case report.
============================================================
Rev Inst Med Trop Sao Paulo 1998 Nov-Dec;40(6):383-5 (ISSN:
0036-4665)
Lambertucci JR; Rayes A; Serufo JC; Teixeira DM; Gerspacher-Lara R;
Nascimento E; Brasileiro Filho G; Silva AC [Find other articles with
these
Authors]
Departamento de Clinica Medica, Faculdade de Medicina da UFMG, Belo
Horizonte, MG, Brazil. [email protected].
We report a case of tropical pyomyositis in a boy who presented with
a
severe febrile illness associated with diffuse erythema, and swelling
in
many areas of the body which revealed on operation extensive necrotic
areas
of various muscles that required repeated debridement. The patient
gave
a
history of contact with dogs, and an ELISA test for Toxocara canis
was
positive. He also presented eosinophilia and high serum IgE levels.
Staphylococcus aureus was the sole bacteria isolated from the muscles
affected. We suggest that tropical pyomyositis may be caused by the
presence of migrating larvae of this or other parasites in the muscles.
The
immunologic and structural alterations caused by the larvae, in the
presence of concomitant bacteremia, would favour seeding of the bacteria
and the development of pyomyositis.
============================================================
33.) [2 cases of toxocariasis (visceral larva migrans)]
[Dos casos de toxocarosis (larva migrans visceral).]
============================================================
Enferm Infecc Microbiol Clin 1996 Nov;14(9):548-50 (ISSN:
0213-005X)
Lopez-Velez R; Turrientes MC; Malo Q; Fenoy MS; Guillen JL [Find other
articles with these Authors]
Unidad de Medicina Tropical y Parasitologia Clinica, Hospital Ramon
y
Cajal, Madrid.
BACKGROUND: Different epidemiological studies have demonstrated that
specific anti-Toxocara antibodies are detected in the serum of a high
percentage of the Spanish population. But very few clinical cases of
visceral larva migrans are being confirmed. METHODS AND RESULTS: Two
cases
of visceral toxocarosis, in two sisters, are described. In the first,
the
prevailing clinic was swelling of joints and upper respiratory tract
symptoms; and asthma and cutaneous allergic manifestations in the second
patient. Both cases presented with an elevated blood eosinophil count,
high
levels of total IgE and high titlers of anti-Toxocara antibodies. All
symptoms disappeared after treatment with diethylcarbamazine and they
remain asymptomatic several months after. CONCLUSIONS: In pediatric
population, toxocarosis should be ruled out in every patient with
respiratory symptoms, allergic cutaneous manifestations and elevated
blood
eosinophil count. The anti-Toxocara antibodies assay is of great value
in
establishing the diagnosis of this parasitic disease.
============================================================
34.) [Visceral larva migrans. A rare cause of eosinophilia in adults]
[Visceral larva migrans. En sjelden arsak til eosinofili hos voksne.]
============================================================
Tidsskr Nor Laegeforen 1996 Sep 20;116(22):2660-1 (ISSN:
0029-2001)
Lund-Tonnesen S [Find other articles with this Author]
Infeksjonsseksjonen Medisinsk avdeling, Haukeland Sykehus 5021, Bergen.
Toxocariasis is a cosmopolitan infection of dogs and cats with a
roundworm
resembling Ascaris. Man becomes infected by ingesting eggs from the
environment. The infection occurs mainly in children. There are two
distinct syndromes: visceral larva migrans and ocular toxocariasis.
The
author describes the case of a 70 year old Norwegian female with
visceral
larva migrans. One month after a visit to Spain she developed fever,
hepatomegaly and marked eosinophilia. Liver biopsy revealed subacute
hepatitis with eosinophilic leucocyte infiltration. Toxocara ELISA
was
strongly positive. Treatment with albendazol 400 mg b.i.d. and
prednisone
10 mg daily for three weeks was successful. A clinical relapse after
three
months was treated in the same way for one month. Prolonged treatment
is
recommended. To our knowledge, this is the first reported case of
visceral
larva migrans in an adult Norwegian. Epidemiology, diagnosis and
treatment
are discussed.
============================================================
35.) [Visceral larva migrans: a mixed form of presentation in an adult.
The
clinical and laboratory aspects]
[Larva migrans visceral: forma mista de apresentacao em adulto. Aspectos
clinicos e laboratoriais.]
============================================================
Rev Soc Bras Med Trop 1996 Jul-Aug;29(4):373-6 (ISSN: 0037-8682)
Barra LA; dos Santos WF; Chieffi PP; Bedaque EA; Salles PS; Capitao
CG;
Vianna S; Hanna R; Pedretti Junior L [Find other articles with these
Authors]
Instituto de Infectologia Emilio Ribas, Instituto de Medicina Tropical
de
Sao Paulo, Brasil.
We relate a case of an 18-year-old man, resident of Xapuri (state of
Acre,
Brazil), with a history of repeated episodes of meningoencephalitis
(three
in one year), each one was examined by a local doctor. In our service
(Emilio Ribas Institute of Infectology) we observed a patient with
polyjoint aches, radiological and bronchoscopic pulmonary alterations
(without clinical features), meningeal and brain stem
manifestations--with
normal brain computed tomography and cerebrospinal fluid. Blood
eosinophils
and serological Toxocara canis test (ELISA) were greatly increased.
With
the hypothesis of Toxocariasis (visceral larva migrans) we administered
thiabendazole that brought complete clinical and laboratory remission.
Inspite of a new episode of headache with meningeal manifestation
approximately one month later (treated with dexamethasone resulting
in a
full remission after three days) we have not found other manifestations
in
approximately three and a half years of ambulatory care.
============================================================
36.) Visceral larva migrans induced eosinophilic cardiac pseudotumor:
a
cause of sudden death in a child.
============================================================
J Forensic Sci 1995 Nov;40(6):1097-9 (ISSN: 0022-1198)
Boschetti A; Kasznica J [Find other articles with these Authors]
Medical Examiner for Suffolk County, Commonwealth of Massachusetts,
Boston,
USA.
A case of fatal cardiac larva migrans in a 10-year-old boy is described.
The autopsy findings were quite dramatic, with a bosselated, sessile
polypoid mass involving the left ventricular myocardium and protruding
into
the ventricular lumen. The precise morphologic characterization of
the
zoonotic ascarid larva was impaired by advanced resorption of the larva
by
an inflammatory infiltrate. Nonetheless, morphometry of the larval
remnants
strongly suggested the raccoon ascarid, Baylisascaris procyonis, as
the
causative agent.
============================================================
37.) [Toxocariasis. A cosmopolitan parasitic zoonosis]
[La toxocarose une zoonose parasitaire cosmopolite.]
============================================================
Allerg Immunol (Paris) 1995 Oct;27(8):284-91 (ISSN: 0397-9148)
Humbert P; Buchet S; Barde T [Find other articles with these Authors]
Service Dermatologie, CHU Saint-Jacques, Besancon.
The infection by Toxocara canis transmitted by dogs (30% of them are
infected in our countries) and less frequently by cats lead to larva
migrans visceral syndrome with neurological manifestations,
ophtalmological
affection and various cutaneous manifestations observed in 24% of the
extra-ocular infections: chronic urticaria often associated with
asthmatic
manifestations and chronic rhinitis, angio-oedema or local oedema
reaching
particularly the eyclid, chronic pruritus associated with lesions due
to
scratching or to nodular prurigo. An hypereosinophilia is an argument
in
favour of a progressive infection. High total IgE is an hallmark of
visceral infections by parasites and total IgE level is well correlated
with the presence of intra-tissular larva. The serological diagnosis
is
based on the determination of specific IgG by ELISA which appears also
to
be interesting for the patient's follow up. The western blot method
seems
to be more specific than the other methods and so is useful to confirm
a
diagnosis. The treatment given as early as possible is based on the
use
of
diethylcarbamazine but also of thiabendazole, albendazole and
mebendazole.
Prophylaxis of toxocara infection includes the prohibition of dog access
to
children games areas but also a frequent turn over of the sand in public
parks.
============================================================
38.) Visceral larva migrans mimicking rheumatic diseases.
============================================================
J Rheumatol 1995 Mar;22(3):497-500 (ISSN: 0315-162X)
Kraus A; Valencia X; Cabral AR; de la Vega G [Find other articles with
these Authors]
Department of Immunology and Rheumatology, Instituto Nacional de la
Nutricion Salvador Zubiran, Mexico City, Mexico.
OBJECTIVE. To report rheumatologic or rheumatologic-like manifestations
of
the visceral larva migrans (VLM) syndrome. METHODS. We carried out
a
prospective study of patients with VLM seen in a private practice
setting
in Mexico City between 1990 and 1993. RESULTS. From a population of
600
patients we identified 6 patients (5 women) with VLM. Three patients
complained of arthralgia; in 4 a history of migratory cutaneous lesions
was
elicited, and in one monoarthritis of the right knee was found. One
patient
had deep edema that suggested thrombophlebitis of the right arm; the
man
in
our series had right testicular swelling during followup. In 2 cases,
panniculitis was documented by biopsy and in one, small vessel
vasculitis.
Four patients had frequent contact with dogs and one with cats; 4
patients
frequently ate raw fish. The diagnosis of VLM was confirmed either
by
the
clinical picture, biopsy, or ELISA. CONCLUSION. The spectrum of
rheumatological manifestations in VLM may be wider than previously
thought.
============================================================
39.) Hepatic granulomas due to visceral larva migrans in adults:
appearance
on US and MRI.
============================================================
Abdom Imaging 1994 May-Jun;19(3):253-6 (ISSN: 0942-8925)
Jain R; Sawhney S; Bhargava DK; Panda SK; Berry M [Find other articles
with
these Authors]
Department of Radio-diagnosis, All India Institute of Medical Sciences,
Ansari Nagar, New Delhi.
Visceral larva migrans is a syndrome characteristically involving
children
with a history of pica, and usually presents with fever, abdominal
pain,
tender hepatomegaly, and hypereosinophilia. Hepatic granulomas of
visceral
larva migrans are rare in adults. We describe three adult patients
with
hepatic lesions which on histopathology demonstrated characteristic
granulomas of visceral larva migrans. All patients had abdominal
sonograms
and two had additional MR scans of the liver. Both ultrasound and
magnetic
resonance imaging demonstrated characteristic appearances which have
not
been described previously (viz., ill-defined central necrotic areas
surrounded by concentric thick walls and perifocal edema in the liver
parenchyma).
============================================================
40.) [Ascaridiasis zoonoses: visceral larva migrans syndromes]
[Zoonoses d'origine ascaridienne: les syndromes de Larva migrans
visceral.]
============================================================
Bull Acad Natl Med 1994 Apr;178(4):635-45; discussion 645-7
(ISSN:
0001-4079)
Petithory JC; Beddok A; Quedoc M [Find other articles with these
Authors]
Department de biologie medicale E. Brumpt Centre Hospitalier, Gonesse.
The syndrome of Visceral Larva Migrans is a zoonotic disease due to
the
migration in human of nematodes larval, specially ascarid. Since the
larvae
fail to complete their migrating cycle in humans, the diagnosis of
Toxocariasis infection remains only serologic. We have been able to
demonstrate by the technique of agar diffusion and the Western-blotting
method that the etiology due to Toxocara canis was twice as much
frequent
as the one due to Toxocara cati in the syndrome of Visceral and Ocular
Larva Migrans. The use of numerous antigens from adult nematodes, mainly
Ascaris suum, has shown, than in France, in the syndrome of VLM at least
12% of the cases were certainly due to other nematodes. Nippostrongylus
brasiliensis (or another similar nematode) of the rat might be
responsible.
The existence of numerous clinical and biological cases found negative
in
serology, allow us to suggest that some other larval nematodes, may
be
from
wild animals, might play an etiological role.
============================================================
41.) Hepatic visceral larva migrans: evolution of the lesion, diagnosis,
and role of high-dose albendazole therapy.
============================================================
Am J Gastroenterol 1994 Apr;89(4):624-7 (ISSN: 0002-9270)
Bhatia V; Sarin SK [Find other articles with these Authors]
Department of Gastroenterology, G.B. Pant Hospital, New Delhi, India.
An unusual presentation of hepatic involvement of visceral larva migrans
is
described. A 45-yr-old male presented with fever, pain in the right
upper
quadrant, and persistent eosinophilia. Ultrasound initially detected
a
solitary hypoechoic area in the right lobe of the liver which rapidly
progressed to multiple lesions with peripheral hyperechoic lesions.
Aspiration from the lesion revealed Charcot-Leyden crystals and sheets
of
eosinophils. Serology for Toxocara canis was strongly positive.
Prolonged
and high-dose albendazole therapy, in combination with antibiotics,
was
required to treat the patient effectively.
============================================================
42.) Neuroimaging studies of cerebral "visceral larva migrans" syndrome.
============================================================
J Neuroimaging 1994 Jan;4(1):39-40 (ISSN: 1051-2284)
Zachariah SB; Zachariah B; Varghese R [Find other articles with these
Authors]
Department of Neurology, University of South Florida College of
Medicine,
H. Lee Moffitt Cancer Center, Tampa, FL.
"Visceral larva migrans" syndrome is a zoonotic disease caused by the
migration or presence in human tissue of nematode larva from lower-order
animals. This syndrome includes generalized illness, eosinophilia, and
symptoms arising from larval invasions of different organs including
the
liver, lungs, eyes, and central nervous system. There has been only
one
case report of the computed tomographic (CT) and magnetic resonance
imaging
(MRI) appearances of cerebral toxocaral disease. Described here is
a
patient with cerebral toxocaral disease with a high eosinophil count
and
toxocaral titer in the serum and abnormal CT and MRI findings who had
spontaneous recovery of the clinical symptoms.
============================================================
43.)[Acute eosinophilic pneumonia and the larva migrans syndrome:
apropos
of a case in an adult]
[Pneumopathie eosinophilique aigue et syndrome de Larva migrans. A
propos
d'un cas chez un adulte.]
============================================================
Rev Mal Respir 1994;11(6):593-5 (ISSN: 0761-8425)
Bouchard O; Arbib F; Paramelle B; Brambilla C [Find other articles with
these Authors]
Clinique de Pneumologie, CHU de Grenoble.
Toxocariasis is a frequent disease in children, but the severe clinical
manifestations are rare in the literature (diffuse interstitial
pneumonia
with hypoxaemia and acute severe asthma). The diagnosis is made thanks
to
the reliability of serological techniques (the ELISA test and using
antigen
excretion-secretion tests of the larvae of Toxocara canis). The authors
report a case of acute severe eosinophilic pneumonia whose outcome
was
rapidly favourable following steroid therapy; the existence of positive
Toxocara canis serology with a contamination risk of the patient in
the
domestic environment leads us to integrate the clinical picture into
the
larva migrans syndrome.
============================================================
44.)Toxocariasis simulating hepatic recurrence in a patient with Wilms'
tumor.
============================================================
Med Pediatr Oncol 1994;22(3):211-5 (ISSN: 0098-1532)
Almeida MT; Ribeiro RC; Kauffman WM; Maluf Junior PT; Brito JL;
Cristofani
LM; Jacob CA; Odone-Filho V [Find other articles with these Authors]
Instituto da Crianca, Hospital das Clinicas, Universidade Estadual
de
Sao
Paulo, Brazil.
We report the case of a 3-year-old girl with stage I Wilms' tumor of
favorable histology. During the course of chemotherapy 5 months
post-diagnosis, an abdominal ultrasonogram revealed hypoechoic areas
consistent with hepatic tumor recurrence. A liver biopsy performed
to
rule
out recurrence of the malignancy was suggestive of toxocariasis and
the
diagnosis was confirmed by serologic testing. Although the patient
had
few
classic signs of visceral larva migrans, her eosinophilia and family
social
history should have suggested this possibility. This case demonstrates
that
hepatic toxocariasis should be considered in evaluating hepatic
hypoechoic
lesions in a child, even when features typical of the disease are
absent.
============================================================
45.) Hepatic imaging studies on patients with visceral larva migrans
due
to
probable Ascaris suum infection.
============================================================
Abdom Imaging 1999 Sep-Oct;24(5):465-9 (ISSN: 0942-8925)
Hayashi K; Tahara H; Yamashita K; Kuroki K; Matsushita R; Yamamoto S;
Hori
T; Hirono S; Nawa Y; Tsubouchi H [Find other articles with these
Authors]
Department of Internal Medicine II, Miyazaki Medical College, Kiyotake,
Miyazaki 889-1692, Japan.
Visceral larva migrans (VLM) is a disease usually observed in children
in
which the larvae of animal parasites invade and reside in human tissues
for
long periods. Although the common causal species of VLM are Toxocara
canis
and T. cati, we identified three adult patients with VLM, probably
due
to
Ascaris suum, whose diagnosis was made by specific immunoserological
tests.
The patients complained of respiratory symptoms, and laboratory tests
showed pronounced eosinophilia, but neither larvae nor eggs were
detected
in stool samples. We present the findings of various imaging studies
of
the
patients. Multiple small hypoechoic mass lesions were demonstrated
by
ultrasound tomography, which disappeared after anti-helminthic therapy.
Hepatic mass lesions were detected as low-density areas on computed
tomography, as high signal intensities on T2-weighted magnetic resonance
images, as space-occupying regions in liver scintigraphy, and as
yellow-white nodules in laparoscopy. Although biopsied liver tissue
specimens showed marked infiltrations of eosinophiles in the portal
tracts
and hepatic sinusoids, neither larvae nor eggs could be identified.
============================================================
46.) Encephalopathy caused by visceral larva migrans due to Ascaris
suum.
============================================================
J Neurol Sci 1999 Apr 1;164(2):195-9 (ISSN: 0022-510X)
Inatomi Y; Murakami T; Tokunaga M; Ishiwata K; Nawa Y; Uchino M [Find
other
articles with these Authors]
Department of Neurology, Kumamoto University School of Medicine, Japan.
We described a patient with encephalopathy associated with visceral
larva
migrans (VLM) caused by Ascaris suum. He suffered from drowsiness,
quadriparesis, eosinophilia and elevated serum IgE levels. Brain
magnetic
resonance (MR) imaging revealed multiple cerebral cortical and white
matter
lesions. Serological tests indicated recent infection with A. suum.
Pulse
steroid therapy relieved the patient's central nervous system symptoms
and
marked improvement of lesions on brain MR images. We concluded that
the
encephalopathy in this patient was probably caused by VLM due to Ascaris
suum.
============================================================
47.) [Imported skin diseases (see comments)]
[Importhuidziekten.]
============================================================
Ned Tijdschr Geneeskd 1998 Dec 12;142(50):2746-50 (ISSN:
0028-2162)
Cairo I; Faber WR [Find other articles with these Authors]
Afd. Huidziekten, Academisch Medisch Centrum/Universiteit van Amsterdam.
In two Dutch subjects who had been on holiday in the tropics, a woman
aged
32 and a man of Surinam descent aged 52 years, and in two men aged
21
and
38 years who had arrived from the tropics in the Netherlands, one
recently
and one 15 years previously, import skin diseases were diagnosed: larva
migrans cutanea, cutaneous leishmaniasis, mycetoma and lobomycosis.
The
diagnosis was based on the anamnesis, the clinical picture and
histopathological findings. The patients were cured by administration
of
antimicrobial agents and (or) excision. When travellers or immigrants
from
the tropics present with skin lesions, an imported skin disease should
be
considered.
============================================================
48.) [Incidence of Toxocara ova--especially ova of visceral larva
migrans
in beach sand of Warnemunde in 1997]
[Studie zum Vorkommen von Wurmeiern--insbesondere von Eiern des
Hundespulwurmes (Larva migrans visceralis-Syndrom) im Strandsand von
Warnemunde 1997.]
============================================================
Gesundheitswesen 1998 Dec;60(12):766-7 (ISSN: 0941-3790)
Schottler G [Find other articles with this Author]
Landeshygieneinstitut Rostock.
Beach sand was examined and analysed in 1997 at several locations in
Warnemunde, a North-East German seaside resort, especially for the
incidence of the nematode genuo Toxocara. Two of 126 samples contained
Toxocara. The author points out measures to decrease the risk of
infection.
============================================================
49.) Pets and Parasites.
============================================================
AU: Juckett-G
AD: West Virginia University School of Medicine, Morgantown, USA.
SO: Am-Fam-Physician. 1997 Nov 1; 56(7): 1763-74, 1777-8
CP: UNITED-STATES
AB: Which parasites can be transmitted by household cats and dogs?
Certainly a variety of potentially dangerous helminths and protozoa
can
be
transmitted to humans from pets but, for the most part, very special
conditions must be present before this occurs. Small children, pregnant
women and immunocompromised persons are three groups at greater
potential
risk than the general population. Infants and toddlers may contract
visceral or cutaneous larva migrans, tapeworm infections and, rarely,
other
helminths or protozoa. Pregnant women and their offspring are at special
risk for toxoplasmosis. Immunocompromised persons (including those with
acquired immunodeficiency syndrome) are susceptible to multiple
infections
but especially to cryptosporidiosis, an underdiagnosed zoonosis present
in
contaminated water supplies. Other zoonotic infections (Echinococcosis,
Dirofilariasis) rarely appear in the general population but, when they
do
occur, pose very real diagnostic challenges. The risk of disease
transmission from pets can be minimized by taking a few simple
precautions
such as avoiding fecal-oral contact, not emptying the cat's litterbox
if
pregnant, washing hands carefully after handling pets, worming pets
regularly and supervising toddler-pet interactions. In most cases,
the
psychologic benefits of pet ownership appear to outweigh the reducible
risks of disease transmission.
============================================================
50.) Cutaneous larva migrans in travelers: synopsis of histories,
symptoms,
and treatment of 98 patients.
============================================================
SO - Clin Infect Dis 1994 Dec;19(6):1062-6
AU - Jelinek T; Maiwald H; Nothdurft HD; Loscher T
PT - JOURNAL ARTICLE
AB - The symptoms, medical history, and treatment of 98 patients
with
cutaneous larva migrans (creeping eruption) who attended a
travel-related-disease clinic during a period of 4 years are reviewed.
This
condition is caused by skin-penetrating larvae of nematodes, mainly
of
the
hookworm Ancylostoma braziliense and other nematodes of the family
Ancylostomidae. Despite the ubiquitous distribution of these nematodes,
in
the investigated group only travelers to tropical and subtropical
countries
were affected; 28.9% of the patients had symptoms for 1 month, and
for
24.5% the probable incubation period was 2 weeks. The efflorescences
typically were on the lower extremities (73.4% of all locations). The
buttocks and anogenital region were affected in 12.6% of all locations,
and
the trunk and upper extremities each were affected in 7.1%. Only a
minority
of patients presented with eosinophilia or an elevated serum level
of
IgE.
No other laboratory data appeared to be related to the disease. Therapy
with topical thiabendazole was successful for 98% of the patients.
Systemic
antihelmintic therapy was necessary in two cases because of
disseminated,
extensive infection.
============================================================
51.) Cutaneous larva migrans.
============================================================
SO - South Med J 1993 Nov;86(11):1311-3
AU - Jones WB 2d
PT - JOURNAL ARTICLE
AB - The case of cutaneous larva migrans presented here is typical
for
its
mechanism and geographic location of infection, evolution of lesions,
and
prompt response to treatment. Except for pinworms, helminth infections
are
rarely thought of in emergency departments away from the areas where
the
parasites are especially prevalent. The several-day incubation period
and
modern-day ease of travel should place this illness on one's list of
the
differential diagnoses of pruritic lesions regardless of the location
of
practice. This case serves as a reminder that in a mobile society,
diseases, as well as patients, can travel.
============================================================
52.)[Current therapeutic possibilities in cutaneous larva migrans]
============================================================
SO - Hautarzt 1993 Jul;44(7):462-5
AU - Wolf P; Ochsendorf FR; Milbradt R
PT - JOURNAL ARTICLE; REVIEW (24 references); REVIEW, TUTORIAL
AB - The recommendations for the treatment of cutaneous larva
migrans
are
not uniform, and the recommended methods are neither always available
nor
always effective. If only the skin is affected, primarily topical
therapy
is indicated. Topical thiabendazole combines efficacy with missing
systemic
side-effects. In Germany the pure substance has to be used or Mintezol
tablets must be purchased from abroad. Topical mebendazole and freezing
with liquid nitrogen are less effective and involve side-effects. If
topical treatment fails, systemic therapy is required. The recognized
treatment with oral thiabendazole (2 days) is associated with numerous
side-effects. There are now two new, safer drugs that should be
preferred:
albendazole (400 mg/day for 3 days), available in Germany as Eskazole,
or
ivermectin (single dose of 200 micrograms/kg). The latter can be ordered
from the manufacturer under the trade name of Mectizan.
============================================================
53.) Cutaneous larva migrans due to Pelodera strongyloides.
============================================================
SO - Cutis 1991 Aug;48(2):123-6
AU - Jones CC; Rosen T; Greenberg C
PT - JOURNAL ARTICLE
AB - A twenty-year-old landscape worker was evaluated for a widespread
cutaneous eruption consisting of papules, pustules, and burrows.
Cutaneous
scrapings revealed live and dead larvae of a free-living soil nematode,
Pelodera strongyloides. This is the third instance of human dermatitis
due
to this organism, and the first reported in an adult host.
============================================================
54.) Oral albendazole for the treatment of cutaneous larva migrans.
============================================================
SO - Br J Dermatol 1990 Jan;122(1):99-101
AU - Jones SK; Reynolds NJ; Oliwiecki S; Harman RR
PT - JOURNAL ARTICLE
AB - Cutaneous larva migrans is becoming more common in the U.K.
with
the
popularity of tropical countries as holiday destinations. We describe
the
increasing use of a new benzimidazole derivative, albendazole, which
is
very effective in the treatment of cutaneous larva migrans. In contrast
to
thiabendazole, it is virtually free from side-effects and should, we
feel,
become the treatment of choice for this condition.
============================================================
55.) Cutaneous larva migrans in northern climates. A souvenir of your
dream
vacation.
============================================================
SO - J Am Acad Dermatol 1982 Sep;7(3):353-8
AU - Edelglass JW; Douglass MC; Stiefler R; Tessler M
PT - JOURNAL ARTICLE
AB - Three young women recently returned to the metropolitan
Detroit
area
with cutaneous larva migrans. All three had vacationed at a popular
club
resort on the Caribbean island of Martinique. Cutaneous larva migrans
is
frequently seen in the southern United States, Central and South
America,
and other subtropical areas but rarely in northern climates. Several
organisms can cause cutaneous larva migrans, or creeping eruption.
The
larvae of the nematode Ancylostoma braziliense are most often the
causative
organisms. Travel habits of Americans make it necessary for
practitioners
in northern climates to be familiar with diseases contracted primarily
in
warmer locations. The life cycle of causative organisms and current
therapy
are reviewed.
============================================================
56.) Creeping eruption. A review of clinical presentation and management
of
60 cases presenting to a tropical disease unit.
============================================================
SO - Arch Dermatol 1993 May;129(5):588-91
AU - Davies HD; Sakuls P; Keystone JS
PT - JOURNAL ARTICLE
AB - BACKGROUND AND DESIGN--Cutaneous larva migrans is an infection
with a
larval nematode, most frequently by dog or cat hookworms. It has a
characteristic presentation that is easily recognizable. We reviewed
the
charts of 60 patients with cutaneous larva migrans who presented to
the
Tropical Disease Unit, Toronto (Ontario) Hospital, during a 6-year
period.
RESULTS--Ninety-five percent of the patients were Canadians who had
recently returned from the tropics or subtropics, notably the Caribbean.
Almost all patients had a linear or serpiginous, very pruritic larval
track. Topical thiabendazole was efficacious in 52 (98%) of 53 patients
treated. Albendazole cured six (88%) of seven patients treated. Because
of
adverse effects, oral thiabendazole and liquid nitrogen were not
utilized.
CONCLUSION--We conclude that topical thiabendazole and oral albendazole
are
very effective and safe modalities for the treatment of cutaneous larva
migrans.
============================================================
57.) Dermatoses associated with travel to tropical countries: a
prospective
study of the diagnosis and management of 269 patients presenting to
a
tropical disease unit.
============================================================
SO - Clin Infect Dis 1995 Mar;20(3):542-8
AU - Caumes E; Carriere J; Guermonprez G; Bricaire F; Danis M;
Gentilini M
PT - JOURNAL ARTICLE
AB - The full spectrum of skin diseases related to travel in
tropical
areas is unknown. We prospectively studied 269 consecutive patients
with
travel-associated dermatosis who presented to our tropical disease unit
in
Paris during a 2-year period. The median age of these patients was
30
years; 137 patients were male; 76% of the patients were tourists; 38%
had
visited sub-Saharan Africa; and 85% had been appropriately vaccinated
against tetanus. Cutaneous lesions appeared while the patient was still
abroad in 61% of cases and after the patient's return to France in
39%.
The
diagnosis was definite in 260 cases; 137 of these cases (53%) involved
an
imported tropical disease. The most common diagnoses were cutaneous
larva
migrans (25%); pyodermas (18%); pruritic arthropod-reactive dermatitis
(10%); myiasis (9%); tungiasis (6%); urticaria (5%); fever and rash
(4%);
and cutaneous leishmaniasis (3%). Hospitalization was necessary in
27
cases
(10%), with a median duration of 5 days (range, 2-21 days). Travelers
should be advised on how to avoid exposure to the agents and vectors
of
infectious dermatoses. Travel first-aid kits should include insect
repellents and antibiotics effective against bacterial skin infections.
============================================================
58.) Larva currens and systemic disease.
============================================================
SO - Int J Dermatol 1984 Jul-Aug;23(6):402-3
AU - Amer M; Attia M; Ramadan AS; Matout K
PT - JOURNAL ARTICLE
AB - Of 26 patients infested with Strongyloides stercoralis 10
(38.5%)
were asymptomatic without systemic or cutaneous signs. Nine patients
(34.6%) presented with systemic complaints only and seven patients
(26.9%)
had systemic and cutaneous manifestations. Further observations of
the
skin
lesions on four of those with systemic and cutaneous manifestations
revealed linear urticarial bands, extending to several centimeters
within 1
hour and persisting up to many days, waiting and waning. Blood
examination
showed eosinophilia in all patients. These findings confirm the concept
that larva currens even alone should be considered a cutaneous sign
of
systemic disease.
============================================================
59.) Hookworm folliculitis.
============================================================
SO - Arch Dermatol 1991 Apr;127(4):547-9
AU - Miller AC; Walker J; Jaworski R; de Launey W; Paver R
PT - JOURNAL ARTICLE
AB - A case of persistent folliculitis in a 21-year-old man was
demonstrated to be due to Ancylostoma caninum larvae. Treatment with
oral
thiabendazole was curative. Cutaneous larva migrans may be due to A
caninum, but this presentation appears to be unique. The literature
concerning etiology and pathogenesis of larva migrans is discussed
with
reference to this case.
============================================================
60.) [Prurigo and further diagnostically significant skin symptoms
in
strongyloidosis]
============================================================
SO - Hautarzt 1988 Jan;39(1):34-7
AU - Bockers M; Bork K
PT - JOURNAL ARTICLE
AB - An increasing incidence of strongyloidosis must be expected
in
European countries as a result of the increasing numbers of immigrants,
as
well as holiday-makers returning from tropical regions. In addition
to
gastrointestinal symptoms, dermatological complaints are predominant.
Only
rarely are cutaneous symptoms the only clinical manifestation of
disease.
The penetration of filariform larvae may cause "ground itch." In cases
of
chronic disease, larva currens is the most obvious sign and consists
of
linear urticarial wheals evoked by larva migration. The most common
non-specific symptoms are rashes, pruritus and urticaria. A further
symptom
of strongyloidosis, intensely itching prurigo, is described in a
20-year-old female Thai. Remission was achieved following tiabendazole
therapy.
============================================================
61.) Gnathostomiasis, or larva migrans profundus.
============================================================
SO - J Am Acad Dermatol 1984 Oct;11(4 Pt 2):738-40
AU - Feinstein RJ; Rodriguez-Valdes J
PT - JOURNAL ARTICLE
AB - Gnathostomiasis, or larva migrans profundus, is a significant
cause
of morbidity in many parts of the world, especially the Far East. Over
forty cases have recently been reported from South America, and some
of
those patients are seeking diagnostic evaluation and treatment in the
United States. A clinical course of painless migratory recurrent
urticarial
skin lesions in a patient who has eaten raw or poorly cooked freshwater
fish should alert a physician to the diagnosis of gnathostomiasis.
============================================================
62.) Visceral larva migrans caused by Trichuris vulpis.
============================================================
SO - Arch Dis Child 1980 Aug;55(8):631-3
AU - Sakano T; Hamamoto K; Kobayashi Y; Sakata Y; Tsuji M; Usui
T
PT - JOURNAL ARTICLE
AB - Two brothers with visceral larva migrans caused by Trichuris
vulpis
were diagnosed after they had been investigated for an eosinophilia.
Both
patients were almost asymptomatic. The diagnosis of visceral larva
migrans
was based on the results of immunoelectrophoretic studies and no liver
biopsy was performed. After administration of thiabendazole, the number
of
eosinophils and serum total IgE levels gradually decreased, and the
patients have remained well.
============================================================
63.) Creeping disease due to larva of spiruroid nematoda.
============================================================
SO - Int J Dermatol 1993 Nov;32(11):813-4
AU - Okazaki A; Ida T; Muramatsu T; Shirai T; Nishiyama T; Araki
T
PT - JOURNAL ARTICLE
============================================================
============================================================
64.) Creeping eruption due to larvae of the suborder Spirurina--a newly
recognized causative parasite.
============================================================
SO - Int J Dermatol 1994 Apr;33(4):279-81
AU - Taniguchi Y; Ando K; Shimizu M; Nakamura Y; Yamazaki S
PT - JOURNAL ARTICLE; REVIEW (13 references); REVIEW OF REPORTED
CASES
============================================================
============================================================
65.) Linear lichen planus mimicking creeping eruption.
============================================================
SO - J Dermatol 1993 Feb;20(2):118-21
AU - Taniguchi Y; Minamikawa M; Shimizu M; Ando K; Yamazaki S
PT - JOURNAL ARTICLE; REVIEW (25 references); REVIEW OF REPORTED
CASES
AB - A 42-year-old woman was referred to our hospital with a
linear
eruption on her right flank of two months duration. Because she had
eaten
loach-fish a month before she noticed the eruption, a creeping eruption
due
to Gnathostoma spp. was initially suspected, but the histological
findings
of the biopsy specimens showed typical features of lichen planus. Linear
lichen planus is discussed based on the cases accumulated in the
literature
regarding the distribution of Blaschko lines.
============================================================
66.) Diagnosis and management of Baylisascaris procyonis infection
in an
infant with nonfatal meningoencephalitis.
============================================================
SO - Clin Infect Dis 1994 Jun;18(6):868-72
AU - Cunningham CK; Kazacos KR; McMillan JA; Lucas JA; McAuley
JB;
Wozniak
EJ; Weiner LB
PT - JOURNAL ARTICLE
AB - Baylisacaris procyonis, the common raccoon ascarid, is known
to
cause
life-threatening visceral, neural, and ocular larva migrans in mammals
and
birds. Two human fatalities have been previously described; however,
little
is known about the spectrum of human disease caused by B. procyonis.
In
this report, the case of a 13-month-old child who had nonfatal
meningoencephalitis secondary to B. procyonis infection is presented.
The
suspected diagnosis was confirmed with use of newly developed enzyme
immunoassay and immunoblot techniques. The diagnosis, management, and
prevention of B. procyonis infection in humans is discussed. Clinical,
serological, and epidemiological evaluations established B. procyonis
as
the etiologic agent. The child survived his infection but continued
to
have
severe neurological sequelae. The potential for human contact and
infection
with B. procyonis is great. There is no effective therapy; therefore,
prevention is paramount.
============================================================
67.) [Human gnathostomiasis. The first evidence of the parasite in
South
America]
============================================================
SO - Ann Dermatol Venereol 1983;110(4):311-5
AU - Ollague W; Ollague J; Guevara de Veliz A; Penaherrera S
PT - JOURNAL ARTICLE
AB - Reporting 4 cases of gnathostomiasis, a clinical review
of this
disease is given by the authors. In one of these cases the diagnosis
could
be established by evidencing the parasite. The name: nodular migratory
eosinophilic panniculitis is suggested for this disease.
============================================================
68.) Efficacy of ivermectin in the therapy of cutaneous larva migrans
[letter]
============================================================
MLID92328556
Author(s) Caumes E; Datry A; Paris L; Danis M; Gentilini M; Gaxotte
P
Source Arch Dermatol 1992;128:994.
Major MeSH Ivermectin ; Larva Migrans
Minor MeSH Administration [Oral]; Adolescence; Middle Age; Prospective
Studies
Check Tag(s) Female; Human; Male
Language English
Pub. Year 1992
Pub. Type Letter
==================================================================
DATA-MEDICOS/DERMAGIC-EXPRESS No 2-(89) 23/02/2.000 DR. JOSE
LAPENTA R.
===================================================================
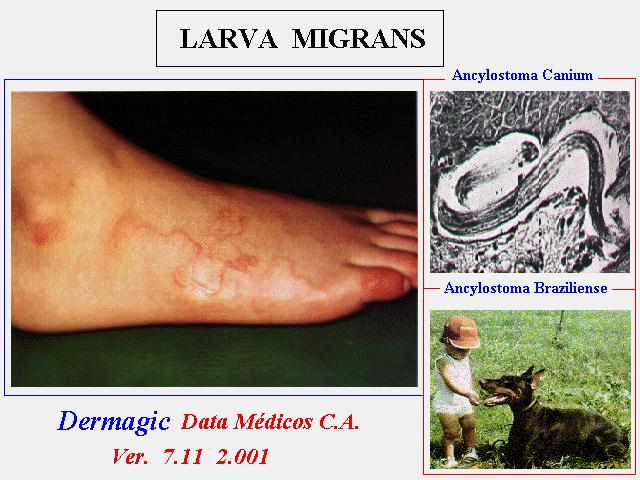
|