3-Hyper mobility and Dislocation:
A-hypermobility:
•Excessive
disc and/or condyle translation usually beyond the eminence
•Usually
associated with
eminence that has
steep short posterior slope followed by a longer
anterior slope and the associated occlusion characterized deep
overbite.
•Clinical
criteria
:
Pain ……… usually no pain unless it becomes habitual.
Tenderness ……. No
Noise………thud (jump
forward to wide opening position )or
popping on
wide opening
sometimes clicking and
this does not occur in lateral excursion.
motion …….excessive and
deviation near the max. opening
may
present
•
N.B. subluxation is a repeatable phenomenon that occur at
the same position even in different speed and force the
position does not change
If there
is clicking it disappear
with function
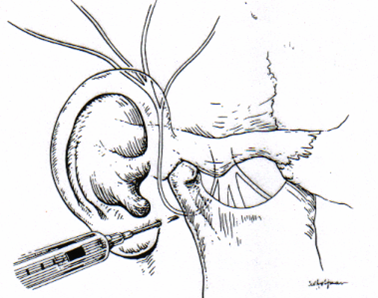
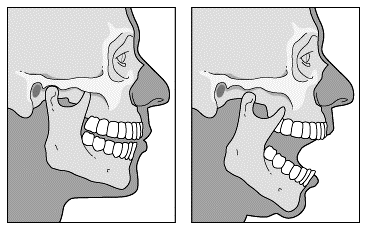
B-Dislocation (open lock):
A
condition in which the condyle is positioned anterior to
articular eminence and can not
return to closed position
•
•Diagnostic
criteria : inability to close the mandible with pain at
the time of dislocation and
residual pain after reduction , trismus usually
associated .
•
•When
the patient can reduce the mandible by himself it is
called hypermobility.
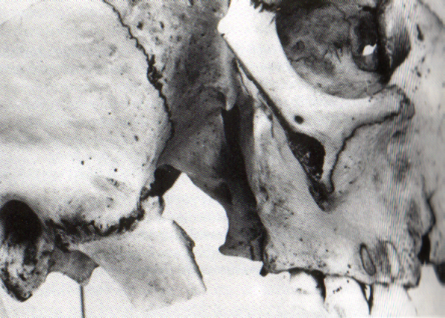
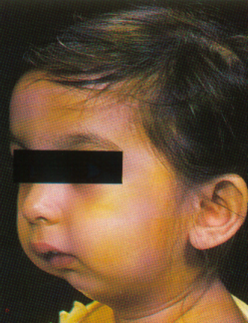
Ankylosis:
•
It is a condition in which fusion of the condyle ,disk and
fossa complex occurs as a result of formation of fibrous
tissue, bone fusion or a combination of the two.
•Ankylosis
may be
fibrous
or
bony
•Clinical
criteria
pain……………no pain
noise………….no joint noise
motion…………marked restriction of mandibular
movement
with deviation to the affected side



Inflammatory articular disorder:
1-Synovitis and capsulitis
•cannot
be differentiated clinically , though not valuable in
treatment.
•Occurs
due to spread of inflammation from adjacent structures ,
infection or trauma
2-arthritides
a- osteoarthrosis
b- osteoarthritis
c- polyarthritides
NON ARTICULAR TMDs:
Keys in differential diagnosis:
1-History
2-Mandibular restriction
3-Mandibular interference
4-Loading the joint
5-Anathetic blockade
CASE 1
•CHIEF
COMPLAINT:
• A
22 years old patient
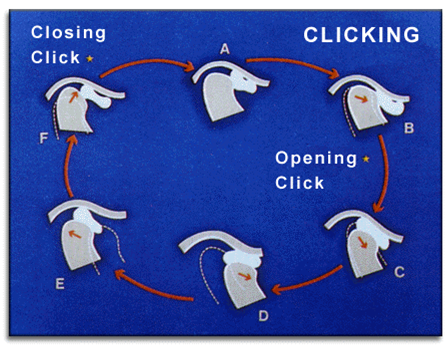
was complaining from left sided TMJ pain and clicking .The
problem began 2 months previously, after the patient was hit
on the jaw. The clicking then started. The pain is well
localized over the TMJ and was worse on eating or talking.
•
•HOW
TO DIAGNOSE
(in steps)
1-Pain
: localized
2-joint
noise: Opening click at 16mm and a
closing click at 4mm
3- range of
motion : The patient opened to 40mm
with deviation towards the left until the opening click
occurred . The mandible then shifted towards the midline.
4-Tenderness:
The left TMJ was tender to palpation and there was left sided
muscle
tenderness
•What
is the diagnosis??
•Case
2:
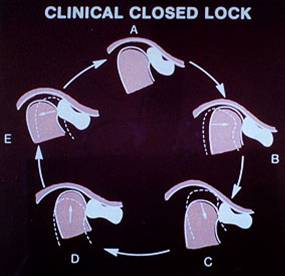
Chief complaint
: Inability to open the mouth wide
•Past
History
: Noise in the right joint for the past 6 weeks which
disappeared suddenly during yawning . Sharp pain
on locking as voluntary opening decreased . Persistent
pain dull and aching.
•
•How
to Diagnose?
•1-Pain:
Sharp pain on locking
•2-Noise:
not present
•3-Motion:
opening 30mm with deviation of the mandible to the right
•4-Tenderness:
localized tenderness of the right TMJ
•
•What
is the diagnosis??
•Case
3:
Chief complaint:
limited voluntary opening , chronic pain in the left joint
,headache
•Past
history
: Grating sounds in the left joint over the past year ,
recurrent dull pain that wakes the patient at night
•
•How
to diagnose?
•1-Pain
: recurrent spontaneous dull pain
•2-Noise:
grating noise
•3-Motion:
limited with deviation to the left on opening
•4-Tenderness:
present in the left shoulder , neck and the masticatory muscle
•
•N.B.TMJ
radiograph positive for joint erosion
•
•What
is the diagnosis??


 \
\