*************************************************************************
2- Allografts:
•
They are grafts
taken from another individual of the same species
•
Because the
individuals are usually genetically dissimilar, the graft is treated to
reduce its antigenicity, usu. It is freeze-dried
3-Xenografts:
•
They are taken from
one species and grafted to another
•
Because
dissimilarity of these grafts is greater they are treated more vigorous to
reduce its antigenicity.
#Alografts &
Xenografts:
•
It is totally
passive, but offers a hard matrix for host site elements to replace
•
It doesn,t require
another site of operation in the host.
# A combination:
A combination of
allogenic graft with autogenous shell was favoured as a way for better
osteoinduction.
4- Alloplastic
materials:
•
Requirements:
–
Adequate Mechanical
properties to withstand cyclic stresses.
–
Non-toxic
–
Non-carcinogenic
–
Immunologically
inert
•
Examples:
–
Hydroxyapatite
–
Tricalcium phosphate
–
Bioactive glass
•
Hydroxyapatite and
other calcium materials are known to
–
1-interact with and
can even incorporate into living bone tissue.,
–
2-they do not
resorb.
–
3-Their
biocompatibility is excellent, and
–
4- they appear to
bond to bone by natural cementing mechanisms & allows for tissue ingrowth
without the formation of a fibrous capsule.
–
5- these materials
are brittle and lack much strength
•
Nonceramic forms
also exist and come as a powder that is mixed in the operating room to
fill bony defects, due to their lack of strength and potential for
fracture, they should not be used in load-bearing areas. This may limit
their use in mandibular augmentation.
#-Modifications:
•
1-Barrier
Membranes:
–
Guided bone
regeneration by covering the graft site by a membrane to exclude
undesirable cell types from the area where bone healing is taking place.
•
2-Osteostimulation:
–
Fifteen residue
peptide(p-15)
–
Recombinant bone
morphogenic proteins(rhBMP-2)
–
Platelet-rich plasma
These biological
materials are used in conjunction with alloplastic materials to stimulate,
enhance or accelerate bone formation at the host site.


******************************************************************

Distraction
Osteogenesis
History of the Procedure:
Distraction was introduced first by Codvilla nearly a hundred years ago
and subsequently was popularized during the 1940s by Ilizarov, who
developed a single-stage procedure to lengthen long bones without the use
of grafting material. However, in the early 1990s, experimental
investigation intensified following reports from New York University on
lengthening of dog mandibles and from Constantino and Friedman et al, who
used DO to successfully close canine segmental lower jaw defects.
Thereafter, several
studies (within a variety of animal models) demonstrated the application
of osteodistraction at a number of different sites including the mandible,
lower maxilla, mid face, and cranial vault. In 1992, the first clinical
results of craniofacial DO were reported by McCarthy et al in a small
series of patients with congenital mandible deformities. Since then,
several larger series with longer follow-up periods have appeared. More
recently, the technique has been successfully used for midfacial and upper
craniofacial skeletal defects.
Method:
The underlying principle
of DO, as described by Ilizarov, is “the mechanical induction of new bone
between bony surfaces that are gradually distracted.” The process of DO
begins with careful preoperative assessment and planning, which are
critical to success. At the initial surgery, osteotomies are performed and
the distraction device is inserted. A waiting period (latency phase) is
allowed to elapse during which bone healing is initiated at the bony gap.
In this early period, periosteal integrity is restored and callus
formation begins. The bone segments at either end of the gap then are
progressively distracted over a period of several days (distraction phase)
during which osteogenesis is induced, thus producing a so-called
regenerate of immature bone laid down between the cut bone ends. Over
time, the bone remodels into a more mature state (consolidation phase),
and the surrounding soft tissues adapt to their new positions and lengths.
•
Tiisues Reaction postoperative:
Bone
remodeling begins during the consolidation phase and continues over 1-2
years, eventually transforming the regenerate into a mature osseous
structure similar in size and shape to the adjacent bone. Although the
volume of new bone is comparable to that of adjacent bones, animal
studies show that mineral content and radiodensity is less
(approximately 30%), as is the tensile strength of the regenerated
segment.
•
There are effects
on the adjacent soft tissue that occur in response to osseous
distraction. Muscle and soft tissue mass increase via a process referred
to as distraction histogenesis. Clinically, this offers a distinct
advantage as several craniofacial anomalies have soft tissue hypoplasia,
in addition to deficient bony structures. Neurovascular elements
contained within distracted bony segments also are stimulated to
regenerate.
•
Problems:
1-patient
noncompliance
2-device
failure
3- premature
fusion of the segments undergoing distraction
These problems
necessitate a repeat surgical procedure to reosteotomize the bone
segments. Infection at the distraction site may impair the osteogenesis
process
During the
consolidation phase
4-nonunion or
delayed union results if micromovement across the regenerate occurs.
5-Excessive
scarring also is possible, particularly when using external devices.
6- A relative
lack of control in repositioning the bone segments exists compared to
conventional surgery, which leads to a less than ideal final position.
•
Several new developments are on the horizon in the field of craniofacial
distraction osteogenesis.
•
Successful
combination of endoscopic techniques to create osteotomies and insert
distraction devices will move distraction into the field of minimally
invasive surgery.
•
New work using
bioresorbable materials may lead to the implementation of devices that
do not require a second surgical procedure to remove them and following
resorption leave no trace that they had ever been inserted.
•
In addition, use
of microprocessors and miniature motorized distraction devices may give
us the ability to insert submerged appliances capable of
auto-distraction according to pre-programmed data.

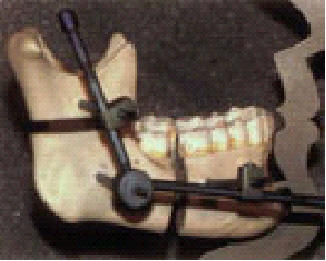

|
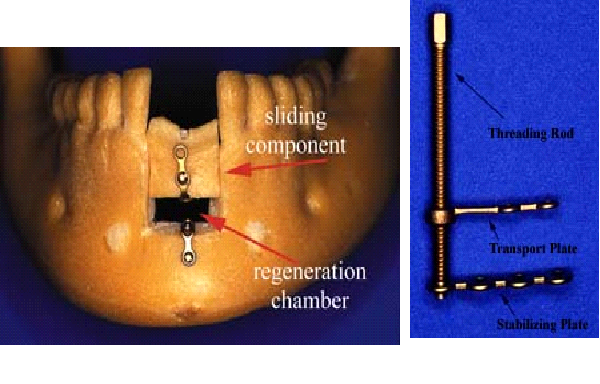
Alveolar Distraction and
its device |



Appendix
1- Bone
physiology
In addition to its
functions of support, Protection and locomotion, bone constitutes an
important reservoir of minerals. Systemically it is cotrolled by hormonal
factors; locally it is controlled by mechanical forces (including tooth
movement), growth factors and cytokines.
Bone Resists
compressive forces best and tensile forces least. It also resists the
forces applied along the axis of its fibrous component; fractures of bone
thus occur most readily as a result of tensile and slicing stresses. (Ten
Cate)
Three Hormones are
primarily concerned with the regulation of calcium metabolism:1,25-Dihydroxycholecalciferol
is a steroid hormone formed from vitamin D. Its primaryaction is to
increase calcium absorption from the intestine, Parathyroid hormone;mobilizes
calcium frombone and increases urinary phosphate excretion, Calcitonin
a calcium-lowering hormone that is secreted primarily by cells in the
thyroid gland and inhibits bone resorption. Glucocorticoids, growth
hormone, estrogen and various growth factors also affect calcium
metabolism, e.g. estrogens prevent osteoporosis, probably by direct
effect on osteoblasts. Insulin increases bone formation and there
is significant bone loss in untreated diabetes. (Ganong)
2-Bone Chemistry
Bone is a
specialized mineral connective tissue consisting by weight of 33% organic
matrix, 28% type I collagen, and 5% non-collagenous proteins; including
osteonectin, osteocalcin, bone morphogenetic proteins, bone proteoglycan
and bone sialoprotein.
This
organic matrix is permeated by the hydroxyapatite Ca10(PO4)6(OH)2,
which makes up the remaining 67% of bone.
Alkaline
Phosphatase enzymeis thought to provide phosphate ions at mineralization
sites. Mineralization is thought to be done by two mechanisms: matrix
vesicle initially, and heterogenous nucleation, where apatite
crystallites are deposited in relation to the collagen fibrils.(Ten Cate)
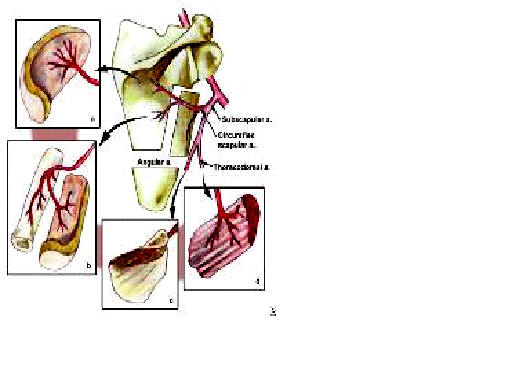
3- Bone Anatomy
Macro-anatomy:
With
maxillary osteotomies, an understanding of the vascular blood supply to
the mobilized maxilla is crucial. The arterial blood supply to the maxilla
is derived from 4 primary sources: (1) the descending palatine branch of
the maxillary artery, (2) the ascending palatine branch of the facial
artery, (3) the anterior branch of the ascending pharyngeal artery from
the external carotid, and (4) the alveolar branches of the maxillary
artery. With complete mobilization of the maxilla, frequently the
descending palatine vessels are disrupted and the mobilized maxilla
derives its vascularity from the remaining sources, primarily the
ascending palatine and pharyngeal vessels.
To
avoid neurosensory deficits with mandibular osteotomies, the surgeon must
be cognizant of the course of the inferior alveolar nerve from its
entrance at the mandibular foramen on the medial aspect of the ramus to
its emergence from the mental foramen between the first and second
premolars. Vertically, the mandibular foramen typically lies approximately
8 mm inferior to the lingula mandibularis (the anterior wall of the
mandibular foramen), and the lingula is approximately 5 mm above the
occlusal plane. With the sigmoid notch as a reference point, the foramen
is approximately 20 mm inferior. Regarding the anterior-to-posterior
relationship, the foramen is located 20 mm from the anterior mandibular
ramal border, a depth of approximately two thirds of the total mandibular
ramal width.
The
canal then courses within the mandible, measuring 2-2.5 mm in diameter.
Its lowest point from the inferior mandibular border is in the region of
the first and second molars, approximately 7.5 mm, before continuing
anterior and superior to its emergence from the mental foramen, where it
is approximately 8 mm from the inferior border. At the mental foramen, the
canal extends caudally before emerging. Regarding the transverse position
of the canal within the mandible, it is most superficial in the region of
the third molar, approximately 2 mm from the buccal plate. In the region
of the first molar, it is 4 mm from the buccal plate
Micro-anatomy:
Types
of bone tissue
Based on texture of cross
sections, bone tissue can be classified as follows: