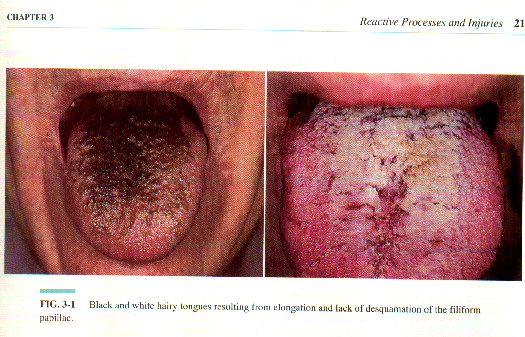
HAIRY TONGUE
Hairy tongue is a common reactive process that results from various precipitating factors including the use of broad-spectrum antibiotics for a systemic infection, radiation therapy for head and neck malignancies, and poor oral hygiene. This tongue abnormality is also observed with much greater frequency in drug addicts, alcohol and tobacco users, and patients infected with human immunodeficiency virus (HIV).
Hairy tongue is rarely symptomatic, although patients may be concerned or disturbed with the unsightly appearance of the lesions. Infrequently, hairy tongue may result ig gagging, halitosis, and taste alterations. desquamation of the papillae can be encouraged by the meticulous oral hygiene and brushing the tongue regularly. Topical application of the retinoids and antifungal medications hastens the resolution of the condition.
CONTACT AND IRRITANT STOMATITIS
Contact stomatitis involving the oral mucosa is well recognized but frequently difficult to diagnose. The oral changes that result from a primary irritant stomatitis may be hard to distinguish from contact stomatitis. Furthermore, the characteristic clinical features of an allergy evident on the skin may be minimal to the mouth. Allergic reactions to acrylic compounds, resins, and metals in dentures, partial dentures, orthodontic appliances, and dental restiration are easily recognized because the mucosal changes are limited to the areas in direct contact with the allergenic material. The allergy manifests as gingival inflammation at the site of contyact between the crown and mucosa. Allergies to foods and chewing gums, topical ancesthetics, and numerous exogenous agents placed in the mouth may result in a burning sensation. Rarely, systemic symptoms and a cutaneous eruption may develop secondary to an oral allergic reaction. The diagnosis of contact stomatitis can be supported by a positive skin test without the need to test the oral mucosa.
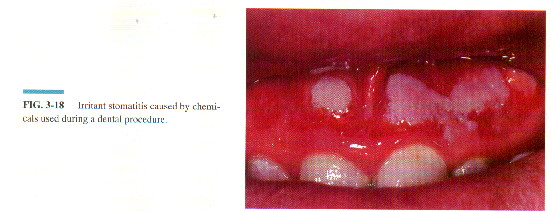
Irritant stomatitis amy commonly develop from the inadvertent contact of various dental chemicals with oral mucosa. For example, phenol, eugenol, bleaching agents, or sodium hypochlorite may cause superficial erosions at their site of contact with the oral mucosa. To achieve pain relief from an aching of tooth, patients frequently apply aspirin preparations directlty on painful teeth and on the adjacent mucosa in the labial or buccal vestibule. This results in the formation o a painful, white, necrotic surface, which desquamates and erodes. Other chemicals applied in the oral cavity may produce similar clinical features. All irritant reactions spontaneously resolve, but the administration of the topical corticosteroids hastens resolution.
DENTURE INJURIES
Denture Stomatitis
Denture stomatitis or denture sore mouths results from the continuous 24-hour-a-day wearing of complete or patial dentures. The condition usually affects tha maxillary alveolar ridge and palate and is clinically characterized by a sharply outlined, deeply reddened, edematous area coinciding with the mucosa directly contacting the denture. Hyperemic pinpoint foce or white patces may be observed within the affected site. The condition is relatively painless, although some patients experience burning. The exact etiology is unknown but is not ussually an allergy to the denture material.
Treatment should be direceted at eliminating candidiasis with topical and possibly systemic agents, depending on the severity, and simultaneously improving oral hygiene.

THERMAL INJURIES
Smoker's Melanosis
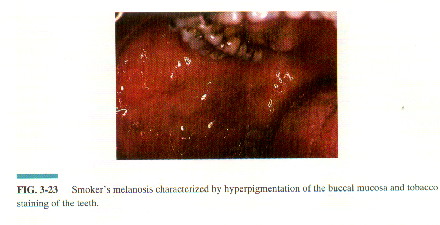
Aside from physiologic pigmentation that is observed in dark-skinned individuals, tobacco use is the most common cause of oral melanin pigmentation. The prevalence of oral pigmentation is significantly higher in smokers who smoke more than 10 cigarettes a day than in nonsmokers, and melanin pigmentation increases proportionately with tobacco consumption.
Smoker's melanosis predominanlty affects the anterior mandibular gingiva and interdental papillae, although pigmentation may also develop on the palate and buccal mucosa. Melanin deposition within the basal cell layer and lamina propria can be demonstrated on biopsy and differentiates this cause of pigmentation from neoplastic processes such as malignant melanoma. The cessation of smoking generally results in disappearance of the pigmentation
Nicotine Stomatitis
Also known as smoker's palate, nicotine stomatitis is a reactive process that occurs almost exclusuvely in long-term pipe smokers. The condition is also observed in reverse smokers(lit end placed in the mouth0, suggesting that thermal effects are responsible for the observed changes. Nicotine stomatitis has a characteristic appearance and is generally confined to the hard palate. Initiall, the palate becomes erythematous before the recognizable changes occur. With continued thermal insult, the mucosa of the palate is transformed into a diffuse, white and thickened surface. The papules on the palate are separated from one another by fissures, creating a wrinkled and rough appearance. The entire process is asymptomatic and is usually discovered during a dental examination. However, nicotine stomatitis in pipe smokers is a benign reactive process that has no malignant potential. cessation of smoking usually results in complete resolution within several months.

