Two of the most common bacterial diseases that afflict humans are dental acrries and periodonatal disease. Streptococcus mutans, the etiologic pathogen of dental caries, and Porphyromonas gingivalis, the bacterial species most strongly associated with adult periodontitis, are inhabitants of the normal flora. In fact, more than 300 different bacteria, including Staphylococcus aureus, coliform bacteria, Klebsiella, and Pseudomonas, reside in the oral cavity and comprise what is regarded as normal oral flora. When species of bacteria increases in number or when the host defense threshold is exceeded, disease arises. In immunocompromised patients, these bacteria may be the source of oral infections that usually manifest clinically as chronic and painful ulcerations or nodules. Life-threatening systemic infections may also be caused by the hematogenous spread of these oral bacteria through ulcerated or inflammed epithelium. Additionally, dental plaque and the oral mucosa are colonized heavily with bacteria that cause nosocomial pneumonia and may be important reservoirs of these pathogens. Even in immunocompetent hosts the potential spread of oral bacteria in patients with endoprosthesis, congenital cardiac malformations, and valvular damage necessitates the prophylactic use of antibiotics before dental or oral surgical procedures. A regimen for adults effective against Streptococcus viridans, the most common oral infectious agent of subacute bacterial endocarditis, is amixicillin, 2g, administered 1 hour before a dental procedure. The oral cavity is also the site of a number of primary bacterial infections and systemic bacterial infections.
GINGIVITIS AND PRIODONTITIS
Periodontal disease is term used to describe disorders of the soft and hard tissues that support the teeth. The bacterially induced inflammatory conditions may involve the gingiva(gingivitis) and the supporting structures including the conectie tissue, periodontal ligament, and alveolar bone(periodontitis).
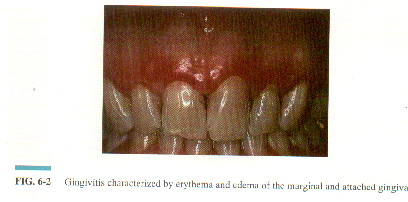
Gingivitis is initiated by the accumulation of dental plaque(the diverse microbial complex on teeth surfaces embedded in a matrix of polymers of bacterial and salivary origin) adjacent to the gingival tissues. The colonization of specific bacteria, primarily the gram-positive cocci Streptococcus sanguis and Streptococcus mitis, occurs initially. If dental plaque control is inadequate, numerous oral bacteria including Actinomyces species and gram-negative organisms colonize the area, resulting in gingival disease. clinically, gingivitis is characterized by erythema, edema, gingival alterations in form and position, and bleeding, especially when the gingiva is brushed or probed.
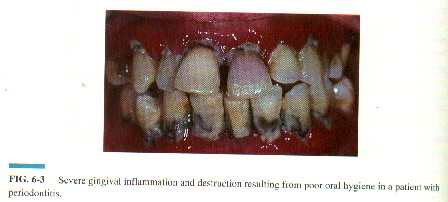
Periodontitis, the most common cause of tooth loss in adults, comprises a diverse group of related but distinct diseases that differ in etiology, natural history, prograsseion, and response to therapy. In all forms, periodontitis is characterized by loss of connective tissue, resorption of alveolar bone, and periodontal pockets. The disease is usually painless and the gingivae coomonly appear healthy, not revealing the destruction of the underlying supporting structures. The detection and diagnosis of periodontitis are based on the abnormal findings of a careful dental examination and radiographs.
SYPHILIS
Syphilis is a sexually transmitted disease caused by the spirochete Treponema Pallidum. During the 1980s the rate of reported cases increased dramatically in part because of drus, prostitution, and HIV infection. Oral lesions are a prominent feature in all stages of syphilis amd may be the first manifestation of the diseaese.
Primary syhilis is characterizedby the presence of a chancre appearing at the site of inoculation approximately 2 to 3 weeks after exposure. Painless ulcerations with firm indurated borders occur equally in frequency or the upper lip and lower lip followed by the tongue, buccal mucosa,a nd the oropharynx.
Secondary syphilis occurs 2 to 10 weeks after the primary lesions has healed. Generalized adenopathy accompanies a widespread eruption, alopecia, and protean systemic symptoms including headaches, arthralgias, lacrimation, and sore throat.
The tertiary stage develops in approximately one third of untreated patients with syphilis, usually 5 to 10 years after the initial infection. Oral lesions occur most commonly during this stage and are characterized by a chronic interstitial glossitis.
Congenital syphilis occurs when spirochetes pass from the placenta to the fetal circulation. During the early stage, usualyy in the first 3 months of life, oral lesions resembling those of acquired secondary syphilis are evident.
The treatment of syphilis consists of intramuscularly administered depot preparations of penicillin.