Candidiasis,synonymously termed candidosis,is the most common infection of the oral cavity with exception of dental cariesand periodontal disease.Moniliasis is an old inaccurate term that has been abandoned.Most cases of oral candidiasis are caused by Candida albicans,although a large number of species of yeasts may be found intraorally.These include C.tropicalis,C.krusei,C.parapsilosis,and C.guillermondii,which are occasionally associated oral infections,especialy in immunocompromised patients.
Candida is a component of the normal oral microflora,which can be isolated in up to one half of otherwise asymptomatic,healthy individuals.The development of an oral infection caused by candida species depends on a complex interaction betweeen the pathogenicity of the organism and the defense mechanism of the host.
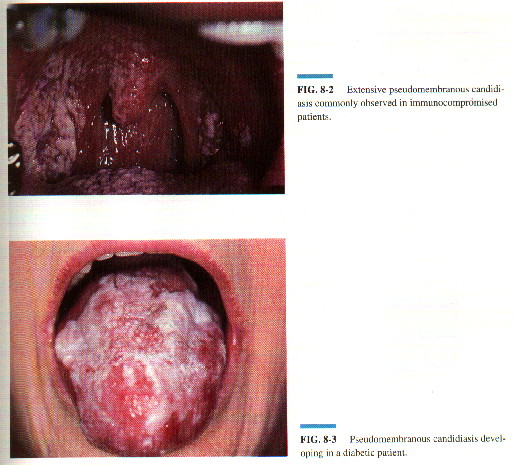
Oral candidiasis can manifest in variety of clinical forms,and the wide diversity can make diagnosis difficult.The most widely recognized pattern is acute pseudomembranous candidiasis or thrush.Although classically observed in infants,patients taking broad-spectrum antibiotics,and debilitated geriatic individuals,pseudomembranous candidiasis is currently detected with great frequency in individuals who are severely immunosuppressed as a result of human immunodeficiency virus(HIV)infection,leukemia,and systematic chemotherapy.The oral infection is charactarized by the development of localized or generalized,loosely adherent white patches and plaques resembling cottage cheese or curdled milk on any or allmucosal surfaces.The white lesions are composed of fungal hyphae, yeast desquamated epithelial cells,and debris.
Erythematous candidiasis refers to a general category of oral candidiasis that encompasses a variety of clinical forms including acute atrophic candidiasis,median rhomboidglossitis,chronic multifocal candidiasis.All of these variants share the absense of superficial,white,curdlike colonies on the oral mucosa and the presence of focal or diffuse areas of erythema with variable symptomatology.
Acute atrophic candidiasis(antibiotic sore mouth)is a frequent complication of broad-spectrum antibiotic use.Patients display diffuse erythema of the oral mucosa,often accompanied by atrophy of the filiform papillae on the dorsal surfaces of the tongue.The lesions are painful and burning.
Median rhomboid glossitis was previously thought to result from faulty involution of the tuberculum impar at the junction of the anterior two thirds and posterior one third of the tongue.Without therapy the lesions frequently resolves spotaneously,but in most cases it remains unchanged and asymptomatic.
Chronic multifocal candidiasis represents a variant media rhomboid glossitis.Multiple areas of atrophic candidiasis,characterized by a red patches and plaques,develop most frequently on the posterior dorsal tongue,at the junction of the hard and soft palates,and in the corners of the mouth.The palatal lesions may result from inoculation from the dorsal surface of the toungue.
Angular cheilitis or perleche may develop as a result of multiple causes including vitamin deficiency and candidal infections.When angular cheilitis is caused by Candida,it ussually occurs in patients with ill-fitting dentures who have lost facial vertical dimensions or who habitually lick the cornrs of their lips.Frequently,patients with angular chelitis have superimpose bacterial infection,usually Staphylococcus aureus.
Chronic atrophic candidiasis may be the most frequently occuring form of oral candidiasis.Affected individuals present with varying degrees of erythema restrictrd to the denture-bearing areas of the mucosa.In contrast to chronic atrophic candidiasis,these reactive prosesses cause pain and acute imflammation of the adjacent mucosa.
Chronic hyperplastic candidiasis or candidal leukoplakia is unique among the forms of oral candidiasis in that plaques cannot be easily scraped or rubbed off.The lesions are generally well-demarcated,white, thick,or verrucous plaques t
Chronic mucocutaneous candidiasis encompasses a heterogenous group of clinical diseases that arecharacterized by chronic candidal infections of the skin,nails,and mucous membranes.In the majority of patients,imunoilogic abnormalities may be demonstrated,although the magnitude and pathogenesis of immunologic defect vary considerably.Chronic candidal infection of the oral cavity is often the initial presenting feature of many of these disorders,endocrinopathies may not maniest for many years, althoughthe sequence may also be reversed.
The clinical diagnosis of oral candidiasis should be confirmed by laboratory tests and can be accomplised by one of several methods.The most common procedure involves digestion of an exfoliative cytologic preparation 10% potassium hydroxide(KOH).
In immunocompetent patients the main treatments for oral candidiasis are topical preparations of nystatin,amphotericin B,miconazole,and clotrimazole.Topical therapy necessities sufficient contact between the drug and oral mucosa.
Systematic therapy with the azole compounds may be required in patients who do not respond to topical hterapy or those with widespread infection.
The use of topical antifungal agents in the preventions of candidiasis in patients undergoing chemotherapy or bone marrow tranplantation in controversial because they may be ineffective.However,the use of systemic agents in this population group is justified in preveting septicemia.In general,correction of the predisposing factors that resulted in oral infection is an important as the specific therapeutic agent.
OPPURTUNISTIC FUNGAL INFECTUIONS
The emergence of newly indentified fungal pathogens and the reemergence of previously uncommon fungal infections are primarily the result of the increased number of susceptible individuals.HIV-infected patients,bone marrow and organ transplant recipients,cancer patients treated with chemotherapy,and very low birth weight infants constitute an immunosuppressed population that is extemely vulnerable to opportunistic fungal infections.The oral cavity is afrequent site of involvement and commonly represents the initial or primary manifestation of a fungal infection.The presence of oral cavity lesions indicates disseminaton of the infection, which necessitates early diagnosis and institution of aggressive therapy.The oral azole drugs,namely,ketoconazole,represent a major advance in systematic antifungal therapy and are effevtive alternatives amtheracin B and flucytosine for selected systemic mycoses.
Aspergillosis
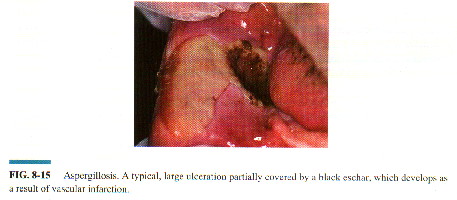
Aspergillus species are ubiquitous and can be detected in soil,water,and decaying vegetation.Infection occurs predominantly in respiratory route,although numerous other locatiojns including the cornea,auditory canal,gastrointestinal tract,nasopharynx,and the skin may be the primary site of infection.Invasive fungal disease develops in predisposed patients who exibit imunosuppression.Profound neutropenia and corcostiroid therapy,especially in leukemia and bone marrow transplant patients,are the greatest risk factors,although a drmatic increase in the number of cases has been recorded in aid patients.
Definitive diagnosis of invasive aspergillosis requires the demonstration of the organismin tissue by histophatology in addition to a positive culture.Special stains such as girdley,methenaminesilvr,or PAS may required to visualized the fungi,which appear as septate hyphae,dichotomously branched at acute angles.Potassium hydroxide preparations,which indicate the presence of a large number of organisms,may be obtained from oral lesions.
The treatment of choice for apergillosis is early aggressive systemic antifungal therapy with amphotericin B and surgical resection of involved tissue.Itraconazole and liposomal amphoteracin preprations are promising new treaments,although resolution of the underlying neutropenia or predisposing factocs may be as important in eradicating the infection.because the majority of oral aspergillosis begins with gingiva,improvement of oral hygiene may prevent infections.