Cysts of the oral cavity and perioral tissues can develop in several ways . All cysts, by definition, are epithelial lined cavities; however, the etiology of oral cysts can be divided into three major categories. Fissural cysts are thoughyt to arise from epithelium that is enclaved during the process of embryonic mesenchymal fusion. Developmental cysts arise from proliferating epithelium within connective tissue in utero, infancy, childhood, or adulthood. The third category contains the odontogenic cysts, which arise in conjunction with developing and erupting teeth.
Although most "developmental" cysts become evedent before adulthood, they all share a common tendency to increase in size gradually, presumably as a result of increased intraluminal hydrostatic pressure with localized bone resorption.
The majority of cysts do not manifests in the oral cavity but are detected radiographically or extraorally during a head and neck examination. The following description of cysts is provided for completeness, with emphasis on oral manifestations.
FISSURAL CYSTS
Palatal Cysts of the Newborn (Epstein's Pearls, Bohn's Nodules)
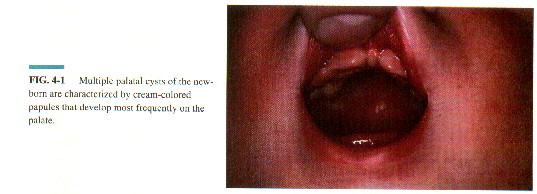
Palatal cysts of the newborn is the consensus term used to describe small developmental systs noted on the palates of the newborn infants. Epstein's pearls were originally described as small cystic lesions arising along the median palatal raphe and were thus fissural in nature. Bohn's nodules are found primarily near the junction of the hard and soft palates and are thought to be derived from minor salivary glands. Because Epstein's pearls and Bohn's nodules are two terms that have been used as interchangeably in the literature and the entities are frequently difficult to distinguish clinically, the term palatal cysts of the newborn is more acceptable.
Palatal cysts pf the newborn are common, present in over two thirds of all neonates examined. The lesions are small, cream-colored papules that are most often found at the junction of the hard and soft palate near the midline. Similar lesions have been reported more anteriorly in the midline of the hard palate, as well as more posteriorly adjacent to the midline.
Palatal cysts of the newborn are keratinizing, as evidenced by their clinical color. No treatment is required because they either degenerates shortly after birth or fuse with the overlying mucosal surface, rupture, and disgorge their contents.
Median Palatal Cysts
The median palatal cyst is a controversial lesion that was proposed to arise from epithelium trapped during the fusion of the lateral maxillary palatal shelves. Most investigators believe, however, that the lesions represents a posteriorly positioned nasopalatine duct cysts rather than a unique entity.
Unlike nasopalatine duct cysts, median palatal cysts are normally seen in younger adults, occasionally attaining a diameter of several centimeters. The histopathologic features of median palatal cysts are identical to those found in nasopalatine duct cysts. They are also treated by surgical excision with minimal risk of recurrence.
VASCULAR-LYMPHATIC LESIONS
Until recently, the nomenclature and classification of vascular birthmarks have been confusing. a new classification of these lesions recognizes two distinct groups taking into account histopathology, pathogenesis, and a natural history. Old terms including cavernous, strawberry, and capillary hemangiomas were descriptive and have been abandoned. The new classification of vascular birthmarks recognizes either hemangiomas or vascular malformations based on their presentation, natural history, and histologic features. A large and diverse group of acquired vascular proliferations in adulthood has been described. This group includes the hemangioma and angioma, as well as various hamartomatous, hyperplastic, and neoplastic tumors. These have not been precisely defined or classified.
Vascular Malformations
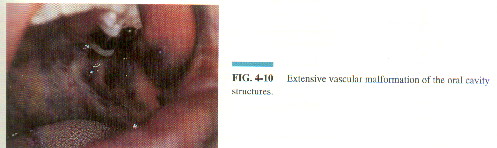
Vascular malformations are always present at birth, never involute. They may be comprised of abnormal capillaries, veins, arteries, lymphatics, or a combination of these. capillary malformations, also known as port-wine stains, are the most frequentlyoccuring cutaneousmalformation and may involve the underlying structuresincluding the ora;l cavity (encephalotrigeminal angiomatosis). Venous malformations andarteriovenous malformations of the oral cavity often go undeteced until adulthood. Whereas venous malformations are low-flow vascular lesions that may require treatment as a result of compression of adjacent structures, arterio-venous malformations are high-flow vascular lesions that may result in ischemia, pain, hemorrhage, and cardiac complications. The latter lesions may be detected by the presence of a pulsating thrill and warmth overlying the lesions, findings that may help differentiate arteriovenous malformations from hemangiomas.
Low-flow oral vascular malformations have been successfully treated with the combination of sclerotherapy and ablative surgery, as well as laser therapy.
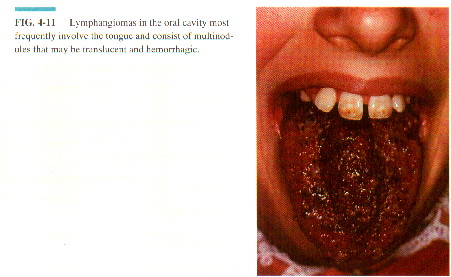
Lymphangioma
Lymphagiomas, like other vascular malformations, are developmental anomalies that occur during embryogenesis. like hemangionesis, these lkesions present with diverse clinical and histologic features ranging from small capillary-size vessels to large cystic lesions with significant involvement of the adjacent anatomic structures.
The vast majority of lymphangiomas occur in the head and neck. Over half of all lymphangiomas are diagnosed at birth, with essentially all lesions being noted clinically by 2 years of age. Extraoral lymphangiomas are more common in the posterior neck. They present clinically as compressible soft tissue masses that have the capacity to undergo significant enlargement, exrending superiorly into the oral cavity and inferiorly to involve the mediastinum. These cystic lymphangiomas, often reffered to as cystic hyrogromas, can resul;t in marked functional impairment and disfigurement.