Alimentary tract and pancreas
Alimentarni trakt i pankreas
Arch gastroenterohepatology 2000; 19 ( no 3 – 4 ):
UNUSUAL CASE OF TERMINAL ILEUM NECROSIS AFTER ACID INGESTION
Neuobicajen slucaj nekroze terminalnog ileuma posle trovanja kiselinom
( accepted November 13th, 2000 )
Terminal ileum acid necrosis
Konstantinos Atmatzidis, Theodoros Pavlidis, Basilios Papaziogas, Ioannis Galanis, Thomas Papaziogas
Second Surgical Department of Medical Faculty of the Aristotles University of Thessaloniki - G Gennimatas Hospital, Thessaloniki, Greece
Address correspondence to: Dr. Basilios Papaziogas
29 Bl.Gabriilidis St.
546 55 Thessaloniki, Greece
E-mail: [email protected]
ABSTRACT
The ingestion of acids leads to epithelial damage of the gastrointestinal tract, which may result in hemorrhage, perforation or necrosis. The intensity of the damage depends on the type, the concentration and the quantity of the ingested liquid. The necrosis on the lower parts of the gastrointestinal tract without concomitant necrosis of the esophagus, stomach or jejunum is extremely uncommon. A case of acid necrosis of the terminal ileum following ingestion of hydrochloric acid solution is presented and the etiology is discussed.
Key words: acid injury, terminal ileum
SAZETAK
Zadesni unos kiselina u alimentarni trakt moze da dovede do hemoragija, nekroze, i perforacije. Intenzitet ostecenja zavisi od tipa, koncentracije, I kolicine unete kiseline. Nekroze distalnih delova gastrointestinalnog trakta bez nekroze I perforacije jednjaka, zeludca, i/ili jejunuma su izuzetno retke. U ovom prikazu se diskutuje slucaj trovanja hlorovoodnicnom kiselinom koja je dovela do nekroze i perforacije terminalnog ileuma.
Kljucne reci: korozivno ostecenje kiselinom, terminalni ileum.
INTRODUCTION
The damages caused after the ingestion of lye concern mainly the upper gastrointestinal tract, i.e. esophagus and stomach. Small intestine is probably protected from injury by two mechanisms: gastric pooling and pylorospasm. Some previous reports called attention to small and large bowel perforations in patients who ingested lye after previous gastric surgery. We report a case of acid necrosis of the terminal ileum after ingestion of hydrochloric acid in a patient with previous subtotal gastrectomy and an unrepaired cleft palate.
CASE REPORT
A 71- year old male patient from a geriatric hospital was admitted to our medical unit six hours after ingestion of a glass of hydrochloric acid solution (over 200 cc) in a suicidal attempt. On examination, he had mucosal burns of the lips, mouth and pharynx and also an unrepaired cleft palate. He had a subtotal gastrectomy with Billroth II reconstruction three years previously. On admission he complained of mild epigastric pain, but there were no clinical signs on the examination of the abdomen. Chest X-ray was normal. His arterial blood pressure was 160/90mmHg and the pulse rate 84 per minute. The patient went on medical treatment (parenteral fluids, antibiotics and cortison). On the evening of the 2nd day he presented with acute epigastric pain and later on, diffuse pain in the abdomen. He underwent emergency laparotomy. At operation, a 30cm long loop of the terminal ileum, 20cm proximal to the ileocecal valve was found to be necrotic. The rest of the small intestine was red and oedematous but the gastric remnant, colon and liver, appeared normal. A resection of the affected loop and an end-to-end anastomosis was performed. The abdomen was drained adequately. The pathology of the resected segment showed rather a chemical necrosis of the small intestine than an ischemic one. (Figure 1)
Postoperatively, the patient was maintained on mechanical ventilation for 48 hours. Following extubation he went on parenteral alimentation. The following days he showed a steadily progressing dysphagia. On the 10th postoperative day he had severe hemmorhage per rectum and passed away three days later from massive bleeding of the GIT and pulmonary insufficiency.
At autopsy, the esophagus and stomach showed numerous circumscribed white areas and the small intestine was red and markedly ulcerated. The trachiobronchial tree was red and oedematous, probably due to a mild degree of lye aspiration caused by the unrepaired cleft palate.
DISCUSSION
The strong irritating nature of acids acting in the upper G.I.T. causes coagulation necrosis of the surface epithelium and the submucosal tissue resulting in chemical esophagitis and gastritis. The intensity of the damaging effect depends on the type of acid, as well as on its concentration and quantity (1,2,3)
The aim of every therapeutic procedure is to preserve homeostatic balance and prevent threatening complications such as schock, airway obstruction, perforation of inner organs or hemorrhage (1,4,5,6)
Acid injury seems to be more superficial in the esophagus than in the stomach, probably because of the rapid passage of acid and the dilution of saliva. (7,8) However, it may lead eventually to perforation of the esophagus. (9,10,11,12) Besides, stricture formation and pulmonary failure are well known complications due to repeated aspiration. At a late stage, carcinoma may develop on the affected area. As far as the stomach is concerned the damage of the columnar epithelium is severe in the antropyloric region. This is probably due to the fact that acid travels along the lesser curvature of the stomach causing marked spasm of the pylorus and prolonging exposure of this area to the acid. Inflammation may lead to multiple ulcerated foci followed, as a rule, by mild or massive hemorrhage. The concentration of the acid and the quantity ingested indicate the intensity of gastric damage. Clinical studies have shown, that there is no relation between the time of contact of the acid and the severity of the lesion of the gastric mucosa.(13,14,15,16)
As far as treatment is concerned, surgical management is still controversial. However, the best procedure for severe cases seems to be a limited or total gastrectomy followed by colonic by-pass of the strictured area of the esophagus. (10,14,16)
The action of acid upon the duodenal wall has also disastrous effects leading often to necrosis of the pancreas, the biliary duct and the mesentery. In such a case, total gastrectomy with splenectomy and resection of the duodenum together with the head of the pancreas, followed by oesophagocolonojejunoplasty has been proposed with good results.(17)
Small intestine and colon are probably well protected from caustic injuries by the above mentioned mechanisms. The development of necrotic changes or perforation of the ileum without concominant damages of the proximal gastrointestinal tract is very unusual (18,19,20,21,22). But in those patients, who have undergone gastrectomy, the acid may pass easily to the small intestine and damage the mucosa causing enteritis, perforation and stricture formation.
There are several reports of colon ingestion of acid in patients with colonoplasty for reconstruction of the esophagus or given accidentally by an enema to otherwise healthy individuals, causing similar damage. (23)
In our case, the competence of the ileocecal valve had probably impeded the passage of the acid into the colon and consequently affected the terminal segment of the ileum.
REFERENCES:
Zarkovic S, Busic I, Volic A. Acute states in poisoning with corrosive substances. Med Arh 1997;51:43-6
Christesen HB. Prediction of complications following caustic ingestion in adults. Clin Otolaryngol 1995; 20(3): 272-8
Christesen HB. Ingestion of caustic agents. Epidemiology, pathogenesis, course, complications and prognosis. Ugeskr Laeger 1997; 155: 2379-82
Stremski ES, Grande GA, Ling LJ. Survival following hydrofluoric acid ingestion. Ann Emerg Med 1992; 21: 1396-9
Gumaste VV, Dave PB. Ingestion of corrosive substances by adults. Am J Gastroenterol 1992; 87(1): 1-5
Kikendall JW. Caustic ingestion injuries. Gastroenterol Clin North Am 1991; 20: 847-57
Jelenko C., Story J., Ellison R. Ingestion of mineral acid. Am Surg 1974; 40: 97-104.
Fisher RA, Eckhauser ML, Radivoyevitch M. Acid ingestion in an experimental model. Surg Gynecol Obstet 1985; 161: 91-9
Stiff G, Alwafi A, Rees BI, Lari J. Corrosive injuries of the oesophagus and stomach: experience in management at a regional paediatric centre. Ann R Coll Surg Engl 1996; 78: 119-23
Broor SL, Kumar A, Chari ST, Singal A, Misra SP, Kumar N, Sarin SK, Vij JC. Corrosive oesophageal strictures following acid ingestion: clinical profile and results of endoscopic dilatation. J Gastroenterol Hepatol 1989; 4: 55-61
Andreoni B, Farina ML, Biffi R, Crosta C Esophageal perforation and caustic injury: emergency management of causticingestion. Dis Esophagus 1997; 10: 95-100
Moulin D, Bertrand JM, Buts JP, Nyakabasa M, Otte JB. Upper airway lesions in children after accidental ingestion of caustic substances. J Pediatr 1985; 106: 408-10
Di-Constanzo J., Cano N., Martin J., Noirlerc M. Surgical approach to corrosive injuries of the stomach. Br J Surg 1981; 68: 879-881.
Chan BS, Duggin GG. Survival after a massive hydrofluoric acid ingestion. J Toxicol Clin Toxicol 1997; 35: 307-9
McAuley CE, Steed DL, Webster MW. Late sequelae of gastric acid injury. Am J Surg 1985; 149: 412-5
Cello JP, Fogel RP, Boland CR. Liquid caustic ingestion. Spectrum of injury. Arch Intern Med 1980; 140: 501-4
Casetti P., Ponzalli M., Dellarolle AC., Duranti A., Favi P., Massimo C. Gastro-duodeno-cefalo-pancreatectomis d’ urgenza per necrosi gastro-duodenale de ingestione de caustici. Minerva Chir 1980; 35: 409-416.
Williamson DW., Hooge WA. Corrosive ingestion: two unusual sites of injury. J Cn Ass Rad 1981; 32: 133-135.
Weintraub BA. A fatal case of acid ingestion. J Emerg Nurs 1997; 23: 413-6
Christesen HB. Diagnosis and treatment of caustic ingestion. Ugeskr Laeger 1994; 156: 4125-8
Schild JA. Caustic ingestion in adult patients. Laryngoscope 1985; 95: 1199-201
Andreoni B, Marini A, Gavinelli M, Biffi R, Tiberio G, Farina ML, Rossi A . Emergency management of caustic ingestion in adults. Surg Today 1995; 25: 119-24
Zavjopodunuv LG. Chemical burns of the rectum and colon in patrurients. Khirurgia 1982; 4: 110-111.
Laugel V, Beladdale J, Escande B, Simeoni U . Accidental ingestion of button battery. Arch Pediatr 1999; 6: 1231-5
FIGURES
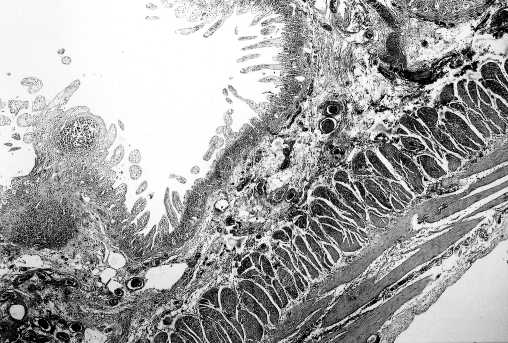
Figure 1. Microscopic view of the resected specimen. Extended necrotic changes of the intestinal wall.