CASE STUDY, PRISTINA, 1994




The
unconscious female patient , 22 years old , has been transferred to the
Department of Endocrinology after the urgent appendectomy had been performed on
the Abdominal Surgery Department, Surgical Clinic, CHC Pristina. She has been
urgently admitted to the Abdominal Surgery department having signs and symptoms
and signs of acute abdomen. The patient is known type 1 diabetic hospitalized
and treated several times in last 5 years at the Department of Endocrinology at
the Clinic for Internal Diseases CHC Pristina.
The
patient started complaining about malaise, frequent urination and fever two
days prior to admission to Surgery. At the evening first day she begun feeling
nausea and during the morning next day she felt pain in the middle and lower
parts of abdomens that have been increasing gradually, becoming very strong in
the evening and she became prostrate and highly febrile.
The
patient and her family then decided to go to the doctor in Pec, where she
lived. During the examination, a doctor
find strong resistance of the anterior abdominal wall on palpation and after
registering leukocytosis (16000/ml) transported the patient by ambulance to
Pristina.
DIFFERENTIAL DIAGNOSIS OF ACUTE ABDOMEN CAN BE FOUND ON:
ENGLISH\CASE 2
WORKUP\Acute abdomen.xps
An
urgent appendectomy was performed. The blood sugar was high (16.7 mmol/l) and
the patient had to receive 250ml 0.9% NaCl + regular insulin 16 j prior to
surgery . She also had 2x 500ml 0.9%NaCl during the operation, and after that
500ml of 10% glucose solution + 16 j of regular insulin. The blood glucose
after the appendectomy was 7.1 mmol/l. During the first day after surgery in
the ED blood glucose levels were 7-10 mmol/l, and the patient received s.c. 6h
– period subcutaneous regular insulin doses matching the actual glucose level.
However, although the anesthesia effect passed she was lethargic and confused.
No
macroscopic signs of appedincitis were seen during surgery and no in-situ signs
of other abdominal diseases were registered. The appendix tissue was sent to
pathologic analysis.
On
the 2nd day in ED, blood glucose continued rising despite
subcutaneous insulin and fluids. On the third day, the patient was transferred
to the department of endocrinology for further treatment.
On
the admission, patient is in stupor, with the reaction (flection) to stronger
physical irritation (pinching, stretching).
She does not react to loud calls but open her eyes slightly during the
physical irritation, and is unable to formulate words but only moans during the
loud calling and in response to pain.
TASK 1: ASSESS CONSCIOUSNESS
IMPAIRMENT USING GLASGOW COMA SCALE
|
Glasgow Coma Scale is provided at
http://www.mdcalc.com/glasgow-coma-scale-score/ |
She
is febrile (38.7C), breathing deeply with the respiratory rate of about 23-25/min
(Kussmaul type). A faint acetone smell is felt in the scent. She is lean, BMI 20.66 kg/m2 (body weight 59 kg, height
1.69m) with no visible deformities. Skin
is pale and dry and mucous membranes are very dry with no visible cyanosis.
The
skull is normally shaped with no visible deformities. The face is symmetric, including eyelids, the
eyes are sunken, conjunctiva and sclera are normally colored but dry, the
pupils react to light symmetrically, but somewhat sluggish. Ears and nose are symmetric, nostrils
movements are normal and the canals are not obstructed. The oral mucous membranes
are dry, the color is normal, upper surface of the tongue is white and coated.
The neck is cylindrical, with no visible deformities. No palpable lymph nodes
on neck were noticed. There is no visible thyroid enlargement, the consistency
during palpation is normal. Thyroid is moving freely during swallowing. The
carotid pulsations are normal, carotid pulse rate is 100/min, but jugular
venous pulse pressure is decreased (hardly palpable).
The
chest wall is cylindrical with no visible deformities. Respiratory movements
are normal, including the intercostal spaces and mobility. Percussion sounds are normal. Respiratory
auscultation reveals normal breathing sounds.
The
heart frequency rate is 100/min, no rhythm disturbances were registered. Heart sounds are normal, no pathologic
murmurs. TA=90/60 mmHg.
The
abdomen is lean with diffuse resistance and tenderness to palpation. Liver span
7 cm in right mid-clavicular line; edge normal, palpable 1 cm above right
costal margin. Bowel sounds are active. Spleen not palpable. There is
postoperative properly dressed wound on the right lower abdominal quadrant. No costo-vertebral angle tenderness is
noted. External genitalia show no
lesions.
Extremities
are cold and without edema. Meningeal signs negative. Flexion movements in response to pain are
symmetrical. Passive resistance to movements is bilaterally normal. No
involuntary movements were recognized. No varicosities, stasis pigmentation or
ulcers on the lower extremities were registered. Arterial pulses on lower
extremities decreased.
TASK 2: CONSIDER THE CAUSES OF DIABETIC KETOACIDOSIS USING:
http://www.mayoclinic.com/health/diabeticketoacidosis/DS00674/DSECTION=causes
Fingertip stick measurement on admission revealed high
blood glucose levels > 25 mmol/l
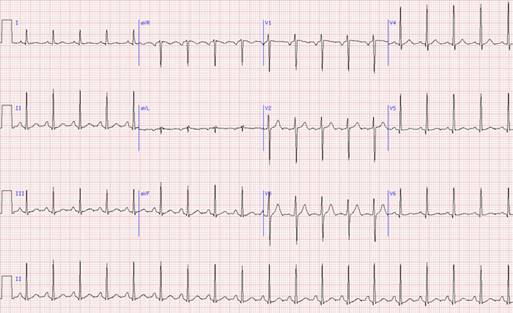
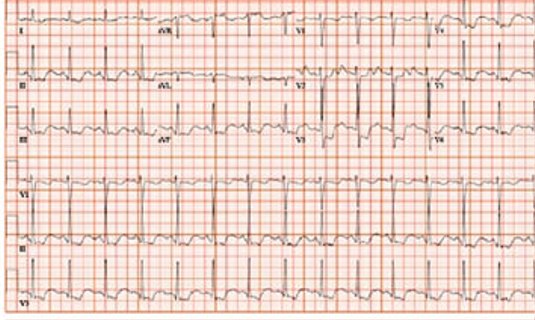
ECG on admission:
RTG on admission:

Abdominal ultrasound

Abdominal
ultrasound: liver normal – 13.5 cm. Portal vein 1.1 cm. gallbladder 2.0 cm, gallbladder wall 1.8mm.
Spleen 12cm. Pancreas could not be seen. Kidneys bilaterally enlarged (15 and
15.5cm, respectively) with mildly enlarged pyelocaliceal structures. Urinary
bladderappears normal.
Laboratory findings on admission:
- The
basic hematologic analysis results (1 h after admission) can be found on:
ENGLISH\CASE
2 WORKUP\Case2 HEMATOLOGIC ANALYSIS 1h.htm
- The
biochemistry analysis results (1h after admission) can be found on:
..\CASE 2 WORKUP\Case2
Biochemical.htm
- The urine
analysis results (1h after admission) can be found on:
ENGLISH\CASE 2
WORKUP\Case2 Biochemical.htm
The referent values of common
biochemistry analyses can be found on
ENGLISH\CASE 2
WORKUP\Case2 URINARY.htm
TASK 3: ASSESS URINE OUTPUT
ml/kg/hour
- The acid-base
parameters analysis(1h after admission) can be found on:
ENGLISH\CASE 2
WORKUP\CASE2 ACIDBASE 1h.htm
- The Serum
lactate and ketone bodies analysis can be found on:
ENGLISH\CASE
2 WORKUP\CASE2 Serum lactate and ketones.htm
The interpretation of the serum lactate
values can be found on:
http://emedicine.medscape.com/article/768159-overview
The interpretation of the serum ketone
values can be found on:
http://type1diabetes.about.com/od/technologyandequipment/p/How-To-Read-Blood-Ketone-Test-Results.htm
http://emedicine.medscape.com/article/2087381-overview
TASK 4: MAKE ASSESSMENT OF
ACID-BASE STATUS USING http://harrisons.unboundmedicine.com/harrisons/ub/view/Harrisons-Manual-of-Medicine/148736/all/acid_base_disorders
- Electrolytes
(1h after admission) can be found on:
ENGLISH\CASE 2
WORKUP\Case2 ELECTROLYTES 1h.htm
TASK 5: CALCULATE SERUM
OSMOLALITY USING:
2Na (mmol/l) + serum glucose (mmol/l) + urea
(mmol/l)
Prior to that, correct serum sodium using
measured Na+ + 0.3 (glucose - 5.5) mmol/
TASK: CALCULATE ANION GAP
USING
Anion Gap = Na - (Cl + HCO3-)
TASK 6: MAKE ASSESSMENT OF
SEVERITY OF DKA USING
ABLE 2
Diagnostic Criteria for Diabetic Ketoacidosis and
Hyperosmolar Hyperglycemic State
|
Mild DKA |
Moderate DKA |
Severe DKA |
HHS |
|
|
Plasma glucose (mg per dL [mmol
per L]) |
> 250 (13.9) |
> 250 |
> 250 |
> 600 (33.3) |
|
Arterial pH |
7.25 to 7.30 |
7.00 to 7.24 |
< 7.00 |
> 7.30 |
|
Serum bicarbonate (mEq per L) |
15 to 18 |
10 to < 15 |
< 10 |
> 15 |
|
Urine ketones |
Positive |
Positive |
Positive |
Small |
|
Serum ketones |
Positive |
Positive |
Positive |
Small |
|
Beta-hydroxybutyrate |
High |
High |
High |
Normal or elevated20 |
|
Effective serum osmolality
(mOsm per kg)* |
Variable |
Variable |
Variable |
> 320 |
|
Anion gap† |
> 10 |
> 12 |
> 12 |
Variable |
|
Alteration in sensoria or
mental obtundation |
Alert |
Alert/drowsy |
Stupor/coma |
Stupor/coma |
DKA =
diabetic ketoacidosis; HHS = hyperosmolar hyperglycemic state.
*—Effective
serum osmolality = 2 × measured Na (mEq per L) + (glucose [mg per dL] ÷ 18).
†—Anion
gap = Na+ – (Cl– + HCO3– [mEq per L]).
Adapted
with permission from Kitabchi AE, Umpierrez GE, Murphy MB, Barrett EJ,
Kreisberg RA, Malone JI, et al. Hyperglycemic crises in diabetes. Diabetes Care
2004;27(suppl 1):S95, with additional information from reference 20.
TASK 7: DOES THE PATIENT NEEDS
INTRODUCTION OF CENTRAL VENOUS LINE
The criteria for installation of CVK are
listed here:
ENGLISH\CASE 2
WORKUP\Case1 CRITERIA CVC.htm
TASK: CALCULATE ANION GAP
USING
Anion Gap = Na - (Cl + HCO3-)
TASK 8: CONFIRM THE INITIAL DIAGNOSIS
OF THE CONDITION USING:
ENGLISH\CASE 2
WORKUP\Case1 HHSvsDKA.htm
TASK 9: CALCULATE TOTAL BODY WATER
DEFICIT USING
TBW deficit (L) = ( 0.6 * Wt * [(Na/140) - 1] )
DIABETIC
KETOACIDOSIS MANAGEMENT HIGHLIGHTS
|
Fluid resuscitation Start 0.9% NaCl at 15–20 mL/kg/hr for first hr (add
colloid if hypovolemic shock), then If Na+ is normal or high, give 0.45% NaCl at 4–14
mL/kg/hr If Na+ is low, give 0.9% NaCl at 4–14 mL/kg/hr Add dextrose when glucose is < 250 mg/dL Goal is to correct total body
water deficit in the first 24 hr |
|
Insulin therapy 0.1 U/kg bolus followed by continuous infusion at 0.1
U/kg/hr Goal is to decrease glucose by 50–75 mg/dL/hr Continue insulin until pH, bicarbonate, and anion gap
normalize Overlap IV insulin with subcutaneous insulin for 1–2
hr after resolution of DKA |
|
Electrolyte repletion Add 20–30 mEq potassium to each liter of IV fluid if
potassium is < 5.3 mEq/L Replace phosphate if phosphate is < 1 mg/dL Give bicarbonate if pH is < 7.0 |
DKA = diabetic ketoacidosis; IV =
intravenous.
TASK 10: PLAN FLUID
RESUSCITATION FOR THE FIRST 6 AND 6-12H.
TASK 11 : PLAN POTASSIUM SUBSTITUTION
FOR FIRST 4 HOURS
TASK 12 : TITRATE I.V. INSULIN
DOSE PER HOUR USING IV INFUSION PUMP OR VIA COUNTING DROPS/MIN USING FOLLOWING
PROTOCOL FOR DIABETIC KETOACIDOSIS.
ENGLISH\CASE 2
WORKUP\Case2 INSULIN.htm
First hour after the
initiation of the therapy
Glucose
23.2 MMOL/L
Urine
output 60 ml
Ta
90/60 mmHg
Second hour
Glucose
21.5 mmol/l
Na++
143 mmol/l
K+ 4.0
P—1.4
Mg++
1.6
TA
95/60 mmHg
Urine
output 75 ml
TASK 13: PLAN THERAPY FOR THE
NEXT HOUR.
Third hour
Glucose
20.0 mmol/l
Na+
142 mmol/l
K+
3,6 mmol/l
Urine
output 80 ml
pH
7.15
PCO2
32
PO2
87
SO2
98%
Serum
bicarbonates 14 mmol/l
Serum
lactate 2.2 mmol/l
Blood
ketones 4.9 mmol/l
3-OH
butyrate 3.0 mmol/l
TA
95/70 mmHg
TASK 14: PLAN THERAPY FOR THE NEXT HOUR
Fourth hour
Glucose
17.1
Na+139
K+
3.95
Urea
9.2
Creatinine
109
Urine
output 85ml
TA
100/65 mmHg
TASK 15: PLAN THERAPY FOR THE NEXT HOUR
Fifth hour
Glucose
15.0 mol/l
Urine
output 85 ml
TASK 16: PLAN THERAPY FOR THE NEXT HOUR
Sixth hour
Glucose
13.7 mmol/l
Na+
139 mmol/l
K+
4.0
pH
7.18
PO2
87
PCO2
33
SO2
98
Serum
bicarbonates 16 mmol/l
Urine
output 90ml
TA
100/70 mmHg
TASK 17: PLAN THERAPY FOR THE NEXT HOUR
Seventh hour
Glucose
12.1 mmol/l
Urine
output 90 ml
TA
110/70 mmHg
TASK 18: PLAN THERAPY FOR THE NEXT HOUR
Eight hour
Na+
140
K+
4.1
pH
7.14
PO2
38
PCO2
33
SO2
97
Serum
bicarbonates 16 mmol/l
Serum
lactate 1.2 mmol/l
Blood
ketones 4.6 mmol/l
3-OH
butyrate 2.8 mmol/l
TA
110/70 mmHg
TASK 19: Despite the good progression in TBW resuscitation, a fall in
serum osmolality, improvement in serum electrolyte levels the fall in serum
ketones, and especially acid base parameters did not correct as expected. During
the 6th hour of therapy the patient became alert, but still drowsy
and ate one banana. However during the eight hour she became lethargic/stuporous
again. What would you do?
Ninth hour
Glucose
11.2
Urine
output 100 ml
TA
115/80 mmHg
The patient suddenly died during the ninth
hour. The exact moment of death was not noted. The reanimation was
unsuccessful. The exact cause of sudden death was not detected, since the
family refused authopsy.
TASK 20: Consider the possible causes of the sudden death