CASE STUDY, MITROVICA, MARCH 2012




Patient
, 43 years old , has been admitted into the ED with the signs of altered
consciousness. He is in stupor, with the reaction (withdrawal) to stronger
physical irritation (pinching, stretching). He reacts to loud calls by opening
his eyes slightly and moaning single words, but is unable to formulate
understandable sentences.
The
patient lived alone. The emergency call was received from the house maid who
came to the apartment twice a week, she could also tell to paramedics that the
patient had diabetes, received tablets for lowering his blood glucose, but was
otherwise well, except that during the last visit when he said to maid he was
not feeling so good and felt tired but otherwise was conscious and mobile.
Because of the increased bodyweight patient’s mobility was rather limited and
he have been going out of his apartment only occasionally with the maid doing
most of the acquisitions required.
She
also provided some medical documentation on visits to the diabetologist one
month ago; the last one shows morning glycemic level 15.2 mmol/l, Hgb A1c 7.5
%, triglyceride 5.7mmol/l, total cholesterol 8.1, HDL 1.36 and LDL cholesterol
5.12 mmol/l. Except for the mild anemia (er 3.500 000/ml, Hgb 105 mmol/l), and
mild leucocitosis (12000/ml), other laboratory tests were within the normal
range. The earlier prescribed therapy contained metformin (Gluformin 500 mg 3x1
tbl.), Cizalapril 5 PLUS (cilazaapril + hydrochlortyazide 17.5 mg) while
sulfonylurea (Predian 2x1 tbl.) and pentoxyfilline (Trental 400mg 2x1) were
introduced during the last visit to endocrinologist. No other known diseases
were known to the maid. Hospital administrative services are about to contact
his relatives and the endocrinologist whom he has been visiting in order to
gain additional data.
TASK 1: ASSESS CONSCIOUSNESS
IMPAIRMENT USING GLASGOW COMA SCALE
|
Glasgow Coma Scale is provided at http://www.mdcalc.com/glasgow-coma-scale-score/ |
The
patient is in stupor, non-febrile, breathing normally with the respiratory rate
of about 18-20/min, obese, his BMI 39 kg/m2 (body weight 115 kg, height 1.71)
with no visible deformities. Skin is pale and dry and mucous membranes are very
dry with no visible cyanosis.
The
patient was in a messy state due to diarrhea with watery stools. He also had
one stool during the transport to the hospital and vomited a little.
The
skull is normally shaped with no visible deformities. The face is symmetric,
including eyelids, the eyes are sunken, conjunctiva and sclera are normally
colored but dry, the pupils react to light symmetrically, but somewhat
sluggish. Ears and nose are symmetric, nostrils movements are normal and the
canals are not obstructed. The oral mucous membranes are dry, the color is
normal, upper surface of the tongue is white and coated. The neck is
cylindrical, with no visible deformities. No palpable lymph nodes on neck were
noticed. There is no visible thyroid enlargement, the consistency during
palpation is normal. Thyroid is moving freely during swallowing. The carotid
pulsations are normal, carotid pulse rate is 100/min, but jugular venous pulse
pressure is decreased (hardly palpable).
The
chest wall is cylindrical with no visible deformities. Respiratory movements
are normal, including the intercostal spaces and diaphragm mobility. There is
some diffuse percussion dullness due to the increased thickness of the fat
tissue on the chest, but no focal changes. Respiratory auscultation reveals
normal breathing sounds.
The
heart frequency rate is 100/min, no rhythm disturbances were registered. Heart
sounds are normal, no pathologic murmurs. TA=90/60 mmHg.
The
abdomen is protuberant. No tenderness or masses were discovered. Liver span 7
cm in right mid-clavicular line; edge smooth, palpable 1 cm below right costal
margin. Bowel sounds are hyperactive. Spleen and kidneys not felt. No
costo-vertebral angle tenderness is noted. External genitalia show no lesions.
Extremities
are cold and without edema. Meningeal signs negative. Withdrawal and flexion
movements in response to pain are symmetrical. Passive resistance to movements
is bilaterally normal. No involuntary movements were recognized. Moderate
varicosities of saphenous veins both lower extremities. No stasis pigmentation
or ulcers. Arterial pulses on lower extremities decreased.
Differential Diagnosis
Our considerations on
differential diagnosis can be found on:
TASK 2: CONSIDER DIFFERENTIAL
DIAGNOSIS USING:
|
http://internamedicina.wikispaces.com/COMA%2C+DIFFERENTIAL+DIAGNOSIS . |
·
Fingertip stick measurement on
admission revealed high blood glucose levels > 25 mmol/l
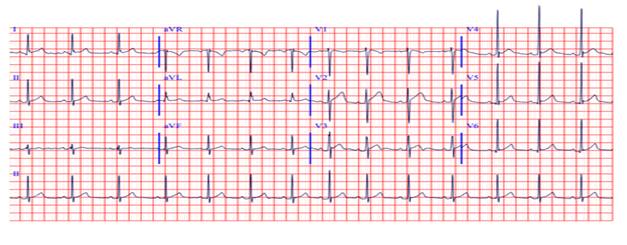
·
ECG on admission:
·
Laboratory findings on admission:
- The
basic hematologic analysis results (1 h after admission) can be found on:
- The
biochemistry analysis results (1h after admission) can be found on:
- The
urine analysis results (1h after admission) can be found on:
The
referent values of common biochemistry analyses can be found on
TASK 3: ASSESS URINE OUTPUT
ml/kg/hour
- The
acid-base parameters analysis (1h after admission) can be found on:
ENGLISH\CASE 1 WORKUP\CASE1
ACIDBASE 1h.htm
- The
Serum lactate and ketone bodies analysis can be found on:
ENGLISH\CASE 1 WORKUP\Serum lactate.htm
- The interpretation of the serum
lactate values can be found on:
http://emedicine.medscape.com/article/768159-overview
- The interpretation of the serum ketone
values can be found on:
http://type1diabetes.about.com/od/technologyandequipment/p/How-To-Read-Blood-Ketone-Test-Results.htm
http://emedicine.medscape.com/article/2087381-overview
http://emedicine.medscape.com/article/2087135-overview#aw2aab6b2
TASK 4: MAKE ASSESSMENT OF
ACID-BASE STATUS USING http://harrisons.unboundmedicine.com/harrisons/ub/view/Harrisons-Manual-of-Medicine/148736/all/acid_base_disorders
- The
serum electrolyte analysis results(1h after admission) can be found on:
ENGLISH\CASE 1 WORKUP\Case1
ELECTROLYTES 1h.htm
TASK 5: CALCULATE SERUM
OSMOLALITY USING:
2Na (mmol/l) + serum glucose (mmol/l) +
urea (mmol/l)
Prior to that,
correct serum sodium using : measured Na+ + 0.3 (glucose - 5.5) mmol/
TASK 6: DOES THE PATIENT
NEEDS INTRODUCTION OF CENTRAL VENOUS LINE
The criteria for installation of CVK are
listed here:
http://www.geocities.ws/urgentnamwu/CASE1/Case1%20CRITERIA%20CVK.htm
TASK 7: CALCULATE ANION GAP
USING
Anion Gap = Na - (Cl + HCO3-)
TASK 8: CONFIRM THE INITIAL DIAGNOSIS
OF THE CONDITION USING:
ENGLISH\CASE 1 WORKUP\Case1
HHSvsDKA.htm
TASK 9: CALCULATE TOTAL BODY
WATER DEFICIT USING
TBW deficit (L) = ( 0.6 * Wt * [(Na/140) - 1] )
TASK 10: CALCULATE WATER/ELECTROLYTE DEFICIT USING:
http://www.geocities.ws/urgentnamwu/CASE1/Case1%20AverageWEdeficit%20HHS.htm
Prior to that,
correct serum sodium using : measured Na+ + 0.3 (glucose - 5.5) mmol/
TASK 11: PLAN FLUID
RESUSCITATION FOR 24h USING:
ENGLISH\CASE 1 WORKUP\Case1 FLUIDsub
HHS.htm
TASK 12: PLAN POTASSIUM SUBSTITUTION
FOR FIRST 4 HOURS USING:
ENGLISH\CASE 1 WORKUP\Case1
POTASSIUMsub HHS.htm
PRINCIPLES OF HHS THERAPY CAN BE FOUND ON: ENGLISH\CASE 1 WORKUP\PRINCIPLES OF HHS THERAPY.htm
First hour after the initiation of the therapy
Glucose
33.2 MMOL/L
Urine
output 65 ml
Ta
90/60 mmHg

NEUROLOGIC EXAMINATION: Patient
stuporous, no lateralizing signs, no pathologic reflexes. Meningeal signs
negative. Dg: Metabolic coma.
TASK 13: PLAN THERAPY FOR THE
NEXT HOUR
The referent
values of common biochemistry analyses can be found on
Second hour
Glucose
33.0. mmol/l
Na++
158 mmol/l
K+ 3.9
P—1.4
Mg++
1.6
TA
95/60 mmHg
Urine
output 75 ml
TASK 14: TITRATE I.V. INSULIN
DOSE PER HOUR USING IV INFUSION PUMP OR VIA COUNTING DROPS/MIN USING FOLLOWING
PROTOCOL FOR DIABETIC KETOACIDOSIS: ENGLISH\CASE
1 WORKUP\Case1 INSULIN.htm
PLAN THERAPY FOR THE NEXT
HOUR.
Third hour
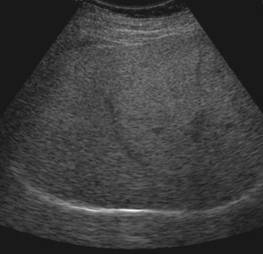

Abdominal
ultrasound: liver moderately enlarged - 17.8cm on MCL, hyperechogenic
(steatotic). Portal vein 1.3 cm. gallbladder 3.0 cm, gallbladder wall 2.8mm.
Spleen 12cm. Pancreas could not be seen. Kidneys bilaterally enlarged (15 and
15.5cm, respectively) but otherwise normal.
Glucose
29.5 mmol/l
Na+ 153
mmol/l
K+ 3,6
mmol/l
Urine
output 80 ml
pH 7.35
PCO2 39
PO2 87
SO2 98%
Serum
bicarbonates 25mmol/l
Serum
lactate 2.8 mmol/l
Blood
ketones 1.7 mmol/l
3-OH
butyrate 1.5 mmol/l
TA
95/70 mmHg
TASK 15: PLAN THERAPY FOR THE
NEXT HOUR
Fourth hour
Glucose
24.1
Na+147
K+ 3.8
Urea
12.8
Creatinine
149
Urine
output 85ml
TA
100/65 mmHg
TASK 16: PLAN THERAPY FOR THE
NEXT HOUR
Fifth hour
Glucose
24.1
Na+147
K+ 3.8
Urea
12.8
Creatinine
149
Urine
output 85ml
TA
100/65 mmHg
TASK 17: PLAN THERAPY FOR THE
NEXT HOUR
Sixth hour
Glucose
21.3 mmol/l
Urine
output 85 ml
TASK 18: PLAN THERAPY FOR THE
NEXT HOUR
Seventh hour
Glucose
17,9 mmol/l
Na+ 146
mmol/l
K+ 4.0
pH 7.38
PO2 87
PCO2 38
SO2 98
Serum
bicarbonates 30 mmol/l
Urine
output 90ml
TA
100/70 mmHg
TASK 19: PLAN THERAPY FOR THE
NEXT HOUR
Eighth hour
Glucose
14.4 mmol/l
Urine
output 90 ml
TA
110/70 mmHg
TASK 20: PLAN THERAPY FOR THE
NEXT HOUR
9. hour
Na+ 144
K+ 4.2
pH 7.38
PO2 38
PCO2 38
SO2 97
Serum
bicarbonates 32 mmol/l
Serum
lactate 3.9 mmol/l
Blood
ketones 1.1mmol/l
3-OH
butyrate 0.9 mmol/l
TA
110/70 mmHg
TASK 21: Despite the good
progression in TBW resuscitation, a fall in serum osmolality, improvement of
the acid-base parameters and serum electrolytes, fall in serum ketones, the
patient is still unconscious, and there is some unexpected rise in serum
lactate levels. What would you do?

10. hour
Glucose
11.2
Urine
output 100 ml
Clotting
factors
Clot
retraction— 75% (normal)
Platelet
aggregation—normal
Fibrinogen
level 3.27 g/l (elevated)
Factor
II— 230% (increased)
Factor
V— 182% (increased)
Factor
VII 130% (normal)
Factor
VIII— 170% (slightly elevated)
Factor
X—120% (normal)
Fibrinogen
degradation products— 7 mcg/L (normal)
TA
115/80 mmHg
Neurologic finding:
The
patient is febrile and exhibited apnoeic phases, along with the , facial
paresis - flattening of the nasolabial fold on left asymmetry of the palpebral
fissures. Left shoulder, arms, wrist and fingers are in hemiplegic position,
leg is extended. (Glasgow Coma Scale score 7).
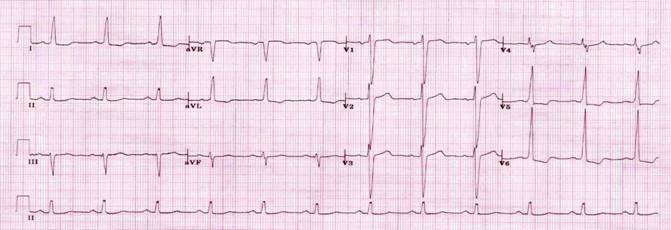
Electroencephalography,
showed a slow basic rhythm consistent with the manifestation of encephalopathy.
CT scan showed right hemisphere ischemic (embolic) stroke.
This course was based on our clinical
experiences and the new recommendations issued by Joint British Diabetes
Societies in August2012. There are also other views on management with the
slight differences comparing to these recommendations, reflecting some
controversial areas in management of HHS. One of the examples is provided on ENGLISH\CASE
1 WORKUP\HHNS management - other views.htm .
TASK 22: COMPARE THE TWO
APPROACHES AND FIND DIFFERENCES