S.A. Patney: InteRyc Volume 4, Oct., Nov. & Dec. 1999
(P.8-11)
STRABISMUS SUMMARY SERIES
NOTE: Only the basic points are covered in this series but they are useful to the
general/pediatric ophthalmologist and the aspiring strabismologist. So far I have not
received any questions and that means one of the two things, either everything is crystal
clear and written beautifully which I doubt. And second possibility is that there isn't
enough interest in the subject. Please let me have the benefit of your feedback.
Visual acuity tests for infants continued:
(The examination of visual acuity is continued from Strabismus Summary - part 1. The first
of the tests in infants (preverbal children), the fixation preference test has already
been discussed. Now we go on to the other tests. As already mentioned in volume 3 of the
InteRyc 1999, only the fixation preference test is widely used clinically. Other tests are
mostly used for research or in better-equipped ocular motility clinics. However, the
basics should be known to every ophthalmologist)
(1) The fixation preference test-variations
(The test was described in Strabismus summary part
1). It is only reliable if the deviation is more than 10 prism diopters. If it is less,
the following tests can be useful.
(1)-a. 10 PD vertical prism test can help by creating a vertical diplopia. If there is
equal visual acuity, equal preference for fixation with either eye will be observed.
(1)-b. 25 PD horizontal prism test can also be performed if the deviation is small or
absent. The eye behind the 25 PD base out prism turns in and its visual acuity is
decreased in that position. Result is a preference for fixation with the other eye. The
prism is then switched over to the other eye. If the eyes can take up the fixation
alternately the visual acuity is approximately equal.
(2) Grating acuity test
These tests include assessment of visual acuity using Teller acuity cards and the forced
preferential looking (FPL) technique. The former can be used as a routine office/clinic
procedure. These cards have parallel black and white stripes of various thicknesses
(spatial frequencies). They are used at 38-cm fixation distance. Resolution acuity is
measured with these cards in cycles per degree. The various cards with broader to narrower
stripes are shown to the infant who sits in the parent's lap and its head movements are
observed. The card with the narrowest stripes, which attracts the baby's attention, is
made note of. Charts with Snellen acuity (recognition acuity) equivalents are available.
The visual acuity as estimated by this method varies from 6/240 at birth, to 6/60 at 3
months of age according to various studies. The visual acuity reaches 6/6 at 3 years of
age*.
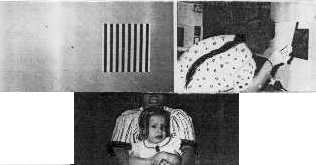
The FPL technique depends on the principle that an infant prefers to look at a pattern
stimulus rather than at a homogenous one (object/surface) as long as the patterned
stimulus is above the threshold of the visual acuity of the infant (figure 1).
|
Figure 1, showing FPL being performed on an infant in her mother's lap. The examiner sits behind the screen, looking through a small hole in the center of the screen. There is a square with a homogeneous surface on one side and another with a patterned surface (black and white stripes) on the other side of the hole in the screen. The examiner watches the head movements of the infant that are caused by looking at the patterned surface in preference to the homogeneous plain surface. |
Suitable age for these tests is upto four months of age as older infants are more liable
to be distracted by the surroundings.
Advantage of these techniques:
These techniques are useful for keeping track of visual development and monitoring of the
visual acuity of the occluded eye during treatment of amblyopia.
(3) Optokinetic nystagmus (OKN)
OKN has been used in research for many years for estimating the visual acuity of infants.
This is yet another objective method.
Nystagmus is produced by showing the infant moving black and white stripes. The narrowest
stripe that still elicits nystagmus is the measure of visual acuity. A handy version of
the equipment is available in the form of a hand-held drum with vertical black and white
stripes (figure 2). The drum is rotated to induce nystagmus.
The visual acuity by this method is stated to be 6/120 at birth according to most studies.
It increases pretty quickly during the first few months after birth.
(4) Visually Evoked Potentials (VEP)
Visual acuity in infants is also estimated using different types of stimuli, cortical
potentials and recording methods. The stimuli used more often are square wave gratings or
checkerboard patterns. The visual acuity by this method has been found to be approximately
6/120 at 1-month age and almost normal adult acuity at 6 months of age according to
various studies.
This technique is now proved to give fairly accurate readings of visual acuity but it
needs expensive equipment and trained technician.
 |
Figure 2, shows the hand-held model of the Optokinetic drum. It is held at 1 foot from the infant and rotated. The visual acuity is indicated by the smallest stripe that can produce nystagmus (by this method 20/200 in a 5 ½ months old). |
Comparison of the above tests: Summing up:
· The fixation preference test is by far the most commonly used test as it is simple and
inexpensive, not requiring any equipment. Moreover, it gives fairly accurate results if
carried out properly.
· Grating acuity methods require a co-operative child and a well-trained and expert
observer. Moreover, grating acuity is always better than recognition acuity (as in Snellen
test), particularly in cases of amblyopia. The Snellen equivalents are only approximate.
(5) Visually Evoked Responses (VER)
The pattern visual evoked response (VER) has been used for estimating the visual acuity in
infants. Its use is an important electrophysiological technique for this purpose. The VER
is a gross response that reflects the visual input from the photoreceptors in the retina
to the occipital cortex, foveal fibres contributing the most.
Most of the studies on this subject indicate that that visual acuity in an infant develops
rapidly so that it reaches the 6/6 (20/20) mark in a 6 months old infant.
A comparison of the VER of the two eyes can help in the early diagnosis of amblyopia. It
can also help in monitoring the occlusion therapy.
NOTE: All these tests give only approximate results. They are not as accurate as methods
using recognition acuity, e.g., Snellen acuity.