The Photograph shows the correct method of holding the infant for the fixation preference test, the covet test and the examination of ocular motility.
The infant is held in the parent's lap unobtrusively so that its head is held straight.
S.A. Patney: InteRyc Volume 3, July, Aug. & Sept. 1999 (P.9-13)
STRABISMUS SUMMARY SERIES
(Note: Only the basic points are covered in this series but they are useful to the
general/pediatric ophthalmologist and the aspiring strabismologist. So far I have not
received any questions and that means one of the two things, either everything is crystal
clear and written beautifully which I doubt. And second possibility is that there isn't
enough interest in the subject. Please let me have the benefit of your feedback. I do work
pretty hard because all this work for the society and the Institute is in addition to my
regular work (practice) and it is pretty disheartening not to know if this series is
serving any useful purpose or not.)
Examination of visual acuity in infants - Part 1
This is a very important subject for obvious reasons. We are not going to repeat here the
usual examination of visual acuity which is carried out everyday in every clinic all over
the world. The main difficulty in assessing the visual acuity is encountered in infants
and young children. The following text enumerates both, the common and not so common
methods of examination of visual function in infants and young (preschool) children:
(1) Tests for infants
(2) Tests in preschool (verbal) children
(1) Tests for infants
(Note: It is obvious that these are all objective tests)
1. Fixation preference test
2. Grating acuity test
3. Optokinetic nystagmus (OKN) test
4. Visual Evoked Potentials (VEP)
(1) 1. Fixation preference test
It is the most useful and commonly used test and supplies a lot of pertinent information
in infants. For this reason this test will be described in some detail. Every
ophthalmologist should be an expert in doing it to be able to detect strabismus and
amblyopia in infants and others. This is in effect a cover test and the only clinical
test, which can supply a lot of useful information regarding the level of visual acuity
and the presence or absence of amblyopia. The infants are unable to perform recognition
tasks.
The other objective tests for young infants described in the next part (InteRyc volume 4,
1999) are usually done only in research laboratories or in exceptionally well equipped
ocular motility clinics.
Even this simple test may prove to be difficult, as infants do not look at any object for
any length of time. It is therefore important to have many interesting fixation objects in
the form of toys, which can attract an infant. Some of them can be with blinking lights,
others that make noise and yet others, which perform amusing, act (animated objects). The
latter can be shown on television monitor screens. In fact many types are available in USA
and the strabismologists or the orthoptists in various motility clinics devise others. I
was amazed at the ingenuity of some of these toys devised by the strabismologists or the
orthoptists. One of the objects Mr. Lyle used often was a bunch of keys. For the reasons
best known to them, most children are very much interested in it. If everything else
fails, a spotlight is used.
The procedure of the fixation preference test is as follows:
1) The infant is seated in mother's or somebody's lap with its back against the chest of
the person holding it (see figure 1). One of the hands of the parent holds the infant's
head while the other arm goes round the baby's trunk.
2) The examiner sits facing them holding an interesting object in front of the infants
face at the level of its eyes in straight line to his nose (primary position) at about
1/3rd of a meter.
3) The fixation behavior of the infant's eyes is then observed keenly.
4) The findings are then recorded in steps in terms "central, steady and
maintained" for the normal fixation behavior as follows:
Step 1: Note down the presence of any abnormal
movements (nystagmus, rapid alternation, binocular searching movements).
Step 2: If a strabismus is present the findings may be either of the two types as given
below:
(a) Easy rapid alternation: Vision in both eyes is
then noted down as " VOU (vision in both eyes): CSM (central, steady and maintained,
the last term describes the fixation behavior when both eyes are open).
(b) One eye may show a unilateral squint, e.g., right esotropia (R ET). The findings are
then noted as "VOS(vision of left eye): CSM.
Step 3: Left eye is then covered and result
observed.
Step 4: Left eye is then uncovered and result observed.
|
Figure 1: The Photograph shows the correct method of holding the infant for the fixation preference test, the covet test and the examination of ocular motility. The infant is held in the parent's lap unobtrusively so that its head is held straight. |
There are various possibilities:
| (A) | The infant protests strongly to covering of the left eye and either moves the head away, removes the cover, starts crying or makes searching movements with the right eye which goes back to the deviating position on removing the cover. The vision is then noted as VOD: UC US UM (uncentral, unsteady, unmaintained) which implies the presence of severe amblyopia with defective fixation. Alternatively, the fixation may be central and the findings are noted as: C US UM (central, unsteady, unmaintained, the latter means the right eye goes back to deviating position). Usually, only C is written and not US UM. |
| (B) | The right eye takes up the fixation and maintains it until the next blink. The result is then noted as VOD: CS (central steady) even if on uncovering the left eye it goes back to the deviating position which is due to the unilateral (right) esotropia (figure 2). |
| (C) | The right eye may go on holding the fixation even when the left eye is uncovered and maintains it beyond the next blink, the vision then is VOD: CSM (central steady maintained). |
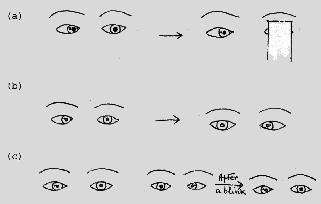 |
Figure 2: (a) R ET with amblyopia and eccentric fixation. (b) A ET (c) R ET - A ET (A = alternating; ET=esotropia) |
Even if technicalities are not observed and one does not wish to bother with all these
details, one can get a lot of information about the infant's visual acuity by remembering
the following points:
| The cover test and the fixation preference test give a pretty good idea of the visual acuity. A quantitative assessment is not possible but unilateral amblyopia can be confirmed or excluded with a fair amount of certainty, as it is the relative vision of one eye as compared to the other, which matters at this stage. | |
| If one looks for more details, one can even have a rough estimate of the level of visual acuity and the degree of amblyopia. This can be done by watching the speed with which the fixation is taken up with an eye and the steady way it is maintained. | |
| If there is free alternation it is safe to presume that the visual acuity is almost equal in both eyes. | |
| If the infant looks with interest at a small object with fine details, the vision is almost certainly good. | |
| If the deviating eye takes up fixation easily when the straight eye is covered and goes back to the deviating position only after holding the fixation for a little while, the vision can not be very poor and amblyopia if present, is not likely to be severe. | |
| The longer the deviating eye takes to take up fixation and the shorter it takes to go back to the deviating position, the poorer is the visual acuity. | |
| Thus the signs of poor visual acuity and presence of amblyopia are as follows: | |
| The infant does not allow the straight eye to be covered (or one of the eyes if there is no strabismus and only anisometropic or some other nonstrabismic amblyopia). | |
| Makes searching movements with the deviating eye. | |
| Fixes eccentrically with it. | |
| Takes a lot of time and effort to fixate an object with it. | |
| Does not keep up the fixation for any length of time and goes back to fixing with the straight eye the moment the covered is removed from that (fixing) eye. | |
| In some cases the infant prefers fixing with one eye, e.g., left but fixates alternately also. This finding of a cover test is noted down as R ET - A ET (RCS - ACS of old which means right convergent squint to alternating convergent squint). This means that any difference in the visual acuity of the two eyes if present is likely to be mild. |
NOTE: All these findings are valid only if confirmed
repeatedly.