 |
 |
 |
Reason # 1 and also the most important reason:
In January of 1996, I suffered a mild stroke and was rushed to the local hospital, which quickly rushed me to a bigger, better hospital, Ohio State University Hospital in Columbus, Ohio. I was transported an hour from home, but it took 3 hours to get there because we were in a level 3 blizzard. It was the longest 3 hours of my life! After many tests, including the grueling TEE (trans esophageal echo) it was determined that the stroke was caused by a hole in my heart called a patent foramen ovale and from a blood clot that had formed at the opening to the hole and a piece of the clot (kinda like dried blood…I don't recall the medical term for it) flaked off and got into my blood stream and blocked the oxygen to my brain. It's a hole that every one of us are born with, but it closes up during development. Mine didn't. But I went all my life not knowing about that until it caused me to have a stroke at the age of 33.
I had waken up from a heavy sleep on my right side to the phone ringing and I couldn't move my right arm…it was paralyzed. My speech was slurred and completely off. Eventually the speech and almost all the feeling came back, but I'm left with very few residual effects as far as sensation of feeling is concerned. The tip of my right thumb is not quite, but almost numb, as is the inside right of my gums and lips. And when I get emotionally upset…it has to be a very upsetting situation, I get very dizzy and if I do too much physically it happens too. I'm very lucky it wasn't worse. I was placed on an anticoagulant, coumadin, and told I would probably be on it for the rest of my life or until I get the hole repaired. Scan to 1999…Cleveland Clinic confirmed the diagnosis and the Neurologists came to the conclusion that they want to put a device in the hole to close it up...a type of double-sided umbrella thing, but I would need to lose a LOT of weight first. That was the deciding factor for me to have this surgery.
In March of 1997 I was in a deep depression after catching my boyfriend cheating on me. I was off work …actually had to drop out of college as I was majoring in Social Work at the Ohio State University Mansfield branch and was just transferring to Ashland University to finish my degree when the stroke happened…and on disability at the time, so I had plenty of time to just sit online trying to get my head together.
I discovered the world of BBWs and their admirers. Again, to shorten a lengthy story, I began going into the BBW chat rooms, making BBW friends, and I started getting a LOT of attention from the kind of men who preferred big women. For the first time in my life that disqualifier was GONE. Finally it was "such a beautiful woman" period. No "if only" attached. I thought I'd died and gone go heaven lol. I started attending BBW-related bashes and other events and made so many friends in women who are just like me. Also..on the down side…for the first time in my life, I had to learn to deal with men who wanted me for just one thing. Imagine that…that was far from the norm up to this point : )
I dated a lot...got played a lot…had my heart broken a lot. BUT it's amazing how all of this patched my self esteem and sent my self worth soaring.
For the first time ever, I felt like it was ok for me to be a big woman. I came to the point of accepting the fact that I would always be a big woman to some degree, even though I knew I needed to be a "smaller big woman"for my health concerns. I had come to realize that it was just my biology to be big and it was finally ok…I stopped apologing to myself and society as a whole especially the popular media for being a "fat chick". I was beautiful as I was. It was wonderful. All that trying to change myself to be loved and accepted was over.
However there was still the fact about the heart needing fixed. And the only way to do that was to lose weight. So I was right about it being ok to be a big person…as long as you are a HEALTHY big person…and yes there are MANY very healthy people who also happen to be big people. I just happened to not be one of them.
So…it's VERY VERY important to me to stress here, that as I have this surgery, this is something I am doing out of medical necessity…so I can have a long and happy life. I would NEVER NEVER do this for purely cosmetic reasons, and I will always always be a BBW inside because that's where my programming is. I will also always be a part of the BBW community..again because that's where my programming is, that's the kind of people I relate to the best and have the most fun with! My only hope in that concern is that the BBW community will be kind to me as I lose the weight. I have already been approached by a few who condemn me for having the surgery saying that they think I can't handle being a BBW and that I am butchering my "beautiful BBW body". This breaks my heart, because as a BBW or BBW Admirer we've come to learn to accept ourselves and love ourselves regardless of size. Note that…REGARDLESS OF SIZE.
Reason # 2 Which is really a long list of reasons:
A list of medical effects of being morbidly obese, some of which pertain to me:
(Borrowed from Dr. Witgrove's site at http://www.gastricbypass.com/B&RSTMO.html -- he's the surgeon who operated on Carnie Wilson)
High Blood Pressure
At least 70% of patients who have high blood pressure, and who are taking medications to control it, are able to stop all medications and have a normal blood pressure, usually within 2 – 3 months after surgery. When medications are still required, their dosage can be lowered, with reduction of their annoying side-effects.
High Blood Cholesterol
Over 80% of patients will develop normal cholesterol levels within 2 – 3 months after operation.
Heart Disease
Although we can't say definitively that heart disease is reduced, the improvement in problems such as high blood pressure, high blood cholesterol, and diabetes certainly suggests that improvement in risk is very likely. In one recent study, the risk of death from cardiovascular disease was profoundly reduced in diabetic patients, who are particularly susceptible to this problem. It may be many years before further proof exists, since there is no easy and safe test for heart disease.
Diabetes Mellitus
Over 90% of Type II diabetics obtain excellent results, usually within a few days after surgery: normal blood sugar levels, normal Hemoglobin A1C values, and freedom from all their medications, including insulin injections. Based upon numerous studies of diabetes and the control of its complications, it is likely that the problems associated with diabetes will be arrested in their progression, when blood sugar is maintained at normal values. There is no medical treatment for diabetes which can achieve as complete and profound an effect, as surgery - which has led some physicians to suggest that surgery may be the best treatment for diabetes, in the seriously obese patient..
Abnormal Glucose Tolerance, or "Borderline Diabetes" is even more reliably reversed by gastric bypass. Since this condition becomes diabetes in many cases, the operation can frequently prevent diabetes, as well.
Asthma
Most asthmatics find that they have fewer and less severe attacks, or sometimes none at all. When asthma is associated with gastroesophageal reflux disease, it is particularly benefited by gastric bypass.
Respiratory Insufficiency
Improvement of exercise tolerance and breathing ability usually occurs within the first few months after surgery. Often, patients who have barely been able to walk, find that they are able to participate in family activities, even sports activities.
Sleep Apnea Syndrome
Dramatic relief of sleep apnea occurs as our patients lose weight. Many report that within a year of surgery, their symptoms were completely gone, and they had even stopped snoring completely – and their spouses agree.
Gastroesophageal Reflux Disease
Relief of all symptoms of reflux usually occurs within a few days of surgery, for nearly all patients. We are now beginning a study to determine if the changes in the esophageal lining membrane, called Barrett's esophagus, may be reversed by the surgery as well – thereby reducing the risk of esophageal cancer.
Gallbladder Disease
When gallbladder disease is present at the time of the surgery, it is "cured" by removing the gallbladder during the operation. If the gallbladder is not removed, there is some increase in risk of developing gallstones after the surgery is performed, and occasionally, removal of the gallbladder may be necessary at a later time.
Stress Urinary Incontinence
This condition responds dramatically to weight loss, usually by becoming completely controlled. A person who is still troubled by incontinence can choose to have specific corrective surgery later, with much greater chance of a successful outcome, with a reduced body weight.
Low Back Pain and Degenerative Disk Disease, and Degenerative Joint Disease.
Patients usually experience considerable relief of pain and disability from degenerative arthritis and disk disease, and from pain in the weight-bearing joints. This tends to occur early, with the first 25 -30 pounds lost, usually within about a month after surgery. Of course, if there is nerve irritation, or structural damage already present, it may not be reversed by weight loss, and some pain symptoms can persist.
We have studied, and recently reported, the relief of the symptoms of co-morbidities in our patients who underwent Laparoscopic Gastric Bypass. For the first 300 patients who underwent that operation, these are the numbers:
I suspect that the person asking this question has never had a serious weight problem in their life and certainly not one that's considered in the "morbidly obese" range. However...
I got the following information from the American Society for Bariatric Surgery from their website at http://www.asbs.org/html/ration.html#RATIONALE
NON-OPERATIVE TREATMENT:
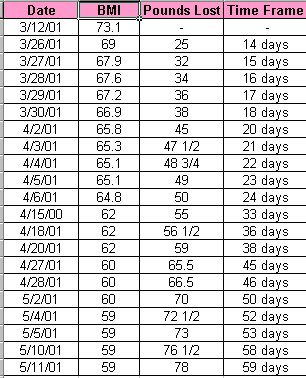
Published scientific reports document that non-operative methods alone have not been effective in achieving a medically significant long term weight loss in morbidly obese adults. {morbid obesity is 100 pounds and more over your ideal weight}.The average medical weight reduction trial is a 10-12 week study with average weight loss of 2.5 kg.(34) The use of anorectic medications has recently been advocated as a long term therapeutic modality in management of what is clearly a chronic disease. In a nearly four year study, utilizing a two drug regimen of Phentermine and Fenfluramine, behavior modification, diet and exercise, the initial optimistic results have not been sustained, with a one third drop out rate and a final average weight loss of only three pounds in those who were followed for the four years of the study.(35) This drug combination appears to have an unacceptably high association with cardiac valvular disease and is no longer recommended. Dietary weight loss attempts often cause depression, anxiety, irritability, weakness and preoccupation with food. The treatment goal for morbid obesity should be an improvement in health achieved by a durable weight loss that reduces life threatening risk factors and improves performance of activities of daily living. Temporary fluctuations of body weight from effective calorie restricted diets should be avoided.
TREATMENT GOALS:
Surgical treatment is medically necessary because it is the only proven method of achieving long term weight control for the morbidly obese. Surgical treatment is not a cosmetic procedure. Surgical treatment of morbid obesity does not involve the removal of adipose tissue (fat) by suction or excision. Bariatric surgery involves reducing the size of the gastric reservoir, with or without a degree of associated malabsorption. Eating behavior improves dramatically.(36) This reduces caloric intake and ensures that the patient practices behavior modification by eating small amounts slowly, and chews each mouthful well. Success of surgical treatment must begin with realistic goals and progress through the best possible use of well designed and tested operations. These have been worked out over the last thirty years, and are now standardized, clearly defined procedures, with well recognized and documented outcome results.
Prevention of secondary complications of morbid obesity is an important goal of management. Therefore, the option of surgical treatment is a rational one supported by the time honored principle that diseases that harm call for therapeutic intervention that is less harmful than the disease being treated. The biological basis for morbid obesity is unknown, though recent work has demonstrated a genetic component of between 25 and 50%, and several studies confirm the influence of genetically determined proteins produced by the fat cell which have a place in the control of satiety. This confirms that morbid obesity is a disease, not a disorder of willpower, as sometimes implied. The physiologic, biochemical and genetic evidence is overwhelming that clinically morbid obesity is a complex disorder. Contributing causes are inheritance, environmental, cultural, socioeconomic and psychological.
