( Post-Op Note: The cardiologist that was monitoring me daily while I was in the hospital told me that he thinks the PFO will close on its OWN as I lose the weight! If that's true and it happens, I won't have to have the device implanted after all!! Pray for me that it does close like he thinks!! :-) )
PFO (Patent foramen ovale) is a persistent opening in the wall of the heart which did not close completely after birth (opening required before birth for transfer of oxygenated blood via the umbilical cord). This opening can cause a shunt of blood from right to left , but more often there is a movement of blood from the left side of the heart (high pressure) to the right side of the heart (low pressure).
Understanding PDAs and PFOs
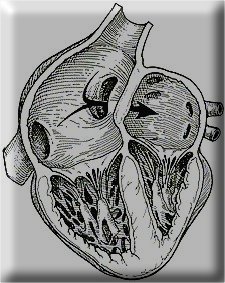
Generally, blood circulates through the body in an endless "figure-eight." One loop carries blood to the lungs to replenish the oxygen, and the other loop carries the oxygen-rich blood to the body. Before we're born, however, things work differently. While in the womb, a child receives oxygen from its mother's lungs. Because it's not breathing, it doesn't need as much blood flowing through its own lungs. So the blood from this loop can be used more efficiently, some of it "takes a shortcut." Instead of going to the lungs, it goes to the rest of the body. There are two shortcuts; normally, both of them close up at birth or shortly thereafter. One shortcut is called the ductus arteriosus. It's a small blood vessel connecting the pulmonary artery and aorta. The other shortcut is called the foramen ovale. It's a small hole between the left and right atria. It's generally higher up, just above where a secundum-type ASD would be located. After birth, the blood pressure increases in the aorta and on the left side of the heart. If either of the two "shortcuts" fails to close up as it should, blood flows through it in the opposite direction, from left to right. These conditions are called Patent Ductus Arteriosus (PDA) and Patent Foramen Ovale (PFO). ("Patent" is a medical term that means "open;" instead of growing shut, these two shortcuts have remained "open.") Either of these conditions can cause symptoms like fatigue, difficult or rapid breathing, failure to grow normally, or chronic respiratory infections. Large openings can lead to heart failure and death. Patent Foramen Ovale
Thanks to http://www.amplatzer.com/patients/pdapfo.html
for a such a good explanation.
Anticoagulant and Antiplatelet Therapies for Patients With PFOs
If patients with PFO have experienced a stroke {That's me!) or transient ischemic attack (TIA), their physician may sometimes recommend a course of therapy that includes anticoagulants or antiplatelet agents. This decision may be made as an alternative to closing the PFO surgically or with a device such as the Amplatzer® PFO occluder.
Among all anticoagulants or antiplatelet agents, Warfarin (also sold as Coumadin) is probably the most widely prescribed drug. While Warfarin is very effective for the prevention and treatment of thromboembolism, it cannot break up blood clots that have already formed nor can it close the heart defect. Furthermore, this drug can sometimes have serious side effects. The likelihood of serious adverse reaction is dramatically increased when interacting with various other drugs. Bleeding such as internal, cerebral and hemorrhoidal bleeding is the most serious complication of oral anticoagulation therapy. Other side effects include necrosis or gangrene of the skin and other tissues, hair loss, purple toes and hypersensitivity reactions.
Careful monitoring is essential to this form of therapy. This is done by measurement of the International Normalized Ratio (INR). This is a ratio of the patient's prothrombin (clotting) time to an international standard. Initially the INR should be checked daily or on alternate days after starting therapy. After hospital discharge, weekly INR estimation is advised for 4-6 weeks. Thereafter, measurement can be extended to every 8 weeks if compliance and control are satisfactory. Changes in the patient's medical condition such as heart disease, thyroid status or drug therapy may alter anticoagulant control and may require more frequent monitoring.
Therefore, when opting for drug therapy over other forms of treatment (i.e. surgical, device closure), one must be ready to accept:
A potential need for life long anticoagulation
Regular visits to the hospital to monitor the INR
Necessity to reduce or eliminate strenuous activities including active sports to avoid injuries which may cause internal or external bleeding (for example, Scuba divers using anticoagulants can sometimes experience bleeding from the ears, sinuses, and lungs)
One other aspect, although probably less important, is the need to avoid leafy green vegetables ( broccoli) which contain significant amounts of vitamin K. Warfarin prevents clots by blocking vitamin K. Eating large amounts of leafy green vegetables that contain vitamin K could prevent Warfarin from doing its job of blocking vitamin K.
Some of the contra-indications to Warfarin therapy include;
Pregnancy - Warfarin is a teratogen (drug that can cause birth defects) and can cause fetal hemorrhage. It should be avoided particularly in the first and third trimester.
Non-thromboembolic stroke
Hemorrhagic conditions
Severe renal and hepatic disease
Hypersensitivity to Warfarin.
In conclusion, for some patients anticoagulant or antiplatelet therapies are potential life-savers. It is however very important to assess the possible risks, side effects and impact that this mode of therapy may have, notwithstanding the impact on the overall quality of life.
To close or not to close, that is the question!
While there is currently no proof for a cause-effect relationship, several recent studies have confirmed a strong association between the presence of a PFO and the risk for paradoxical embolism or stroke. When compared with control subjects, the relative risk of suffering a thromboembolic event is four times as high in patients with PFO; it's 33 times as high in patients with both PFO and atrial septal aneurysm. Furthermore, a widely patent foramen (>5mm separation) and a severe shunt (< 50% of the left atrium filled with contrast) have been identified as echocardiographic predictors of an increased risk for paradoxical embolism in a recent retrospective study.
In addition, there is good evidence that patients with PFO and paradoxical embolism are at increased risk for future, recurrent cerebrovascular events. A retrospective French multicenter study reported a yearly risk of 1.2% to sustain a recurrent TIA, and of 3.4% to suffer a recurrent stroke or TIA; this was despite medical treatment with oral anticoagulants or antiplatelet drugs in patients with PFO and cryptogenic stroke. Similarly, in the Lausanne study the stroke recurrence rate among 140 patients with PFO and stroke amounted to 1.9% per year, whereas the combined stroke and TIA recurrence rate was 3.8% per year.
The presence of PFO or atrial septal aneurysm has no therapeutic consequence in otherwise healthy adults. In contrast, patients suffering a stroke or TIA in the presence of a PFO and without another cause of ischemic stroke are considered for drug therapy to reduce the risk of a recurrent embolic event. As mentioned earlier, patients are commonly treated with oral anticoagulants or antiplatelet agents. To date, however, there is no consensus on which treatment (oral anticoagulation versus antiplatelet therapy) is superior, or on how long medical treatment should be continued after the index event. Several randomized studies between anticoagulants or antiplatelet agents and transcatheter closure devices are currently underway both in the United States and in Europe in order to answer that question.
In the mean time, more and more physicians trust the added benefits of transcatheter closure of PFOs using the Amplatzer® PFO Occluder. The device offers a simpler, less invasive alternative to traditional surgical methods. It also allows patients to avoid the potential side effects often associated with anticoagulation therapies. More importantly it aims at sealing the defect thus eliminating permanently the passage of thrombi through the communication.
This is a picture similar to the device they want to implant into my heart to close the hole (the PFO). It's described to be like a double-sided umbrella and each side goes on either side of the opening of the PFO. The only difference is, that as it was explained to me the "umbrella tops" are made of dacron
Thanks to AGA Medical Corporation for this image
Click HERE to see a movie of how the device is implanted through a catheter that is inserted into the artery in the groin.
Other Links regarding the Patent Foramen Ovale:
http://www.amplatzer.com/demos/deploy/pfo.html
http://www2.umdnj.edu/~shindler/foramen_ovale.html
http://www-medlib.med.utah.edu/WebPath/CVHTML/CV115.html
Cleveland Clinic's Echocardiogram Movies showing the PFO:
http://www.clevelandclinic.org/heartcenter/echo/cases/preclip00017.htm

