|
DE TRADUS SI CITAT
Nursing99 March
1999
This continuing-education offering is sponsored by Sage
Products Inc. and provided by The Nursing Institute
Quickly and easily assessed, your patient's mouth speaks volumes about his
condition. Here's how to "listen" and respond. See
Assessing the mouth.
Contrary to what you may have heard, oral complications arising from a
disease or treatment are not inevitable burdens that your patient has to
bear. Instead, these conditions are frequently preventable and treatable.
In this handbook, you'll learn about the situations and clinical conditions
that pose the greatest risk of oral problems. You'll also learn who's most at
risk for these problems and how to prevent or manage them. First, though, let's
review the anatomy of the mouth.
Layers of the Oral Mucosa

Understanding oral anatomy
Oral mucosa. The oral mucosa is continuous, from the edge of the lips
(mucocutaneous junction) at the proximal end to the wet epithelial lining of the
digestive tract at the distal end. The oral mucosa has three layers: the outer
layer or epithelium, the middle layer or lamina propria, and the inner layer or
submucosa. (See Layers of the Oral Mucosa.)
The epithelium is self-renewing. Stem cells of its deepest area replicate and
differentiate to form the various cells of the surface epithelium. These cells
have a life span of 3 to 5 days, so the outer epithelial layer is replaced about
every 7 to 14 days.
This rapid cellular renewal ensures the integrity of the oral mucosa. It also
provides an effective barrier against both exogenous and endogenous
microorganisms, including gram-positive and gram-negative bacteria, fungi, and
viruses. In healthy patients, the resident flora pose no systemic threat; in
fact, they help control the colonization of exogenous microorganisms in the
mouth.
During normal functioning, the oral mucosa is subject to frequent traumas.
Mostly these result in microulcers that are asymptomatic and heal uneventfully.
More serious traumas--such as those from food burns, accidental biting, or
mechanical injury--produce larger ulcers that, although painful, heal
spontaneously in 10 to 14 days. Repeated exposure to extraneous sources of
irritation or cellular damage, such as radiation or chemotherapy, produces
extensive inflammation of the oral mucosa, a condition called mucositis or
stomatitis. (For the characteristics of a healthy mouth, see
Keeping Score: A Numeric
Gauge of Your Patient's Oral Health.)
Saliva. Each day, the salivary glands produce 800 to 1,500 ml of
nonviscous, slightly acidic saliva (pH, 6.0 to 7.4). Saliva contains large
quantities of bicarbonate and potassium. Secreted at 0.5 ml/minute, saliva keeps
the oral mucosa moist, smooth, clean, and shiny. It also maintains a balance of
microbial flora and preserves the teeth's mineral integrity.
Saliva's components contribute to its maintenance functions. For example, the
protein mucin removes debris, dead cells, and the waste products of cellular
metabolism. Large glycoproteins in the saliva bind to the oral mucosa and reduce
the adhesion of microorganisms. The salivary peroxidase process uses saliva's
components to initiate an oxygenation process that inhibits the growth of
microorganisms.
Tongue. With 10,000 or so taste buds, the tongue can detect myriad
flavors--though it requires saliva to do so because taste buds respond to
substances in solution. Taste changes when the taste buds degenerate or are
absent, saliva is inadequate, the sense of smell isn't intact, or certain
organic substances circulate in the bloodstream.
Gums and teeth. The gums (or gingiva) consist of squamous or
parakeratinized epithelium and underlying fibrous connective tissue. They attach
to the neck of the tooth; the attachment's integrity is a major factor in
gingival and periodontal disease.
Tooth enamel--the tooth's surface--resists erosion by acids, enzymes, and
acid-producing microorganisms. When the enamel isn't adequately cleaned, plaque
(debris containing bacteria and fungi) collects and adheres to the tooth's
surface, especially at the neck. As the plaque accumulates, the gingiva becomes
inflamed, then recedes and separates from the tooth. Pockets develop, allowing
additional plaque to accumulate and destroy adjacent fibers and bone. This
progressive destruction is called periodontal disease; in a compromised patient
(for example, one who is debilitated or has an immune disorder), it can be a
significant source of sepsis.
Bacteria on the teeth also produce acids that decalcify the enamel, creating
cavities (or caries). Untreated, caries allow bacteria to penetrate the tooth
and inflame the underlying tissues, causing severe pain and leading to
inflammation or infection of adjacent bone or soft tissue. The infection can
then spread to contiguous sites of the body, including the cavernous sinus and
the brain. Because the microorganisms can directly access the blood and
lymphatic vessels that supply the tooth, localized infections can become
systemic, especially in compromised patients.
At-risk factors
Who's at risk for oral problems? Here are a few general situations to watch
for, no matter what your patient's illness or injury may be.
1. The presence of an endotracheal tube, which is a constant irritant
to the oral cavity. A patient with an endotracheal tube requires frequent
assessment and scrupulous care to prevent ulcers, bleeding, and infection. The
tube also makes oral care difficult to perform.
Although suctioning an intubated patient removes saliva and debris, the
suctioning appliances are normally hard and abrasive and can cause trauma to a
compromised oral cavity. The appliances have to be cleaned after every use to
avoid bacterial contamination. Within 48 hours of intubation, a patient can be
colonized with bacteria that can cause pneumonia.
2. A history of inadequate oral hygiene or poor nutrition
3. Use of the following drugs:
 | reserpine, chlorpromazine, cholinergic blocking agents (such as atropine
and belladonna), and antihistamines--can cause a decrease in salivary flow
|
| phenytoin--can cause gingival hyperplasia
|
| antibiotics--can deplete the mouth's normal protective flora, allowing
opportunistic pathogens to proliferate
|
| antineoplastic drugs and biologic response modifier (BRM) therapy--can
alter the oral mucosa's integrity and ability to regenerate. |
4. Other situations or injuries:
| oxygen therapy--increases the evaporation of moisture from the tongue and
mucous membrane
|
| tachypnea--causes dry mouth (xerostomia) because the saliva is humidifying
the inspired air more quickly than it can be produced
|
| mouth breathing--may eliminate the normal fluctuating pressures necessary
to stimulate blood circulation in gingiva tissues
|
| oral or nasogastric suctioning
|
| N.P.O. status
|
| a diet rich in hot or coarse foods, such as pretzels, chips, or crackers
|
| poorly fitting dentures
|
| exposure to tobacco or alcohol. |
Troubled trio
Keeping these general situations in mind, let's discuss three patient groups
that are likely to have oral complications: the elderly, cancer patients, and
patients with human immunodeficiency virus (HIV) disease.
Elderly patients. The normal degenerative changes of aging such as
diminished keratinization of the mucosa, atrophy of the tongue, unusual or
unpleasant taste perceptions (dysgeusia), and decreased saliva production place
the elderly at risk for oral problems. Gingivitis also increases with age: In
one study, 90% of people ages 75 to 90 had moderate to severe gingivitis. Many
elderly people wear dentures, which, combined with the above factors, can also
increase their risk.
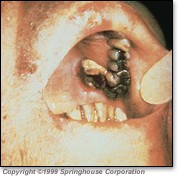
Photo 1: Squamous cell carcinoma
 Cancer patients. Cancer
causes major depression of the immune system, making mouth infections more
likely. This likelihood increases if cancer cells have infiltrated bone marrow
or if radiation therapy or chemotherapy compromise the marrow's ability to
produce white blood cells. Various cancer cells may infiltrate the oral mucosa,
causing infarction with sloughing that blocks oral mucosal capillaries. Mouth
tumors disrupt the mucosa's integrity and are frequently infected, necrotic, and
painful. (See Photo 1.) Cancer patients. Cancer
causes major depression of the immune system, making mouth infections more
likely. This likelihood increases if cancer cells have infiltrated bone marrow
or if radiation therapy or chemotherapy compromise the marrow's ability to
produce white blood cells. Various cancer cells may infiltrate the oral mucosa,
causing infarction with sloughing that blocks oral mucosal capillaries. Mouth
tumors disrupt the mucosa's integrity and are frequently infected, necrotic, and
painful. (See Photo 1.)
The common forms of cancer treatment--radiation, chemotherapy, and bone
marrow transplant--pose a significant threat to the mouth. Surgery involving the
head and neck also increases risks significantly. Other surgeries pose indirect
threats because of the accompanying physical trauma, changed breathing patterns,
decreased self-care, and nutritional loss.
Like surgery, radiation directly affects the oral cavity only when it
involves the head and neck. When these sites are the target of radiation
therapy, mucositis usually appears 1 to 2 weeks after treatment begins and
continues for several weeks after it ends. Radiation aimed at other areas of the
body won't directly affect the oral mucosa, but the adverse effects (anorexia,
nausea, vomiting, and diarrhea) produce nutritional losses that affect the
mouth.
Chemotherapy has a harmful impact on the mouth on two counts. First, it
targets actively replicating cells, so the oral mucosa's stem cells are
particularly vulnerable to destruction. Second, it interferes with DNA, RNA, or
protein synthesis, reducing production of the mucosa's epithelial cells,
impairing their differentiation, and accelerating detachment. As the mucosal
cells slough off, the mucosa becomes thin, fragile, and vulnerable to even minor
trauma, paving the way for inflammation and infection. If the patient is
thrombocytopenic, expect bleeding as well.
Photo 2: Chemotherapy-induced stomatitis
 Among the chemotherapeutic agents,
those most likely to cause stomatitis are the antimetabolites and antineoplastic
antibiotics. The antimetabolites include cyclophosphamide (Cytoxan), cytosine
arabinoside (Ara-C), 5-fluorouracil (5-FU), floxuridine, 6-mercaptopurine
(6-MP), methotrexate, and 6-thioguanine. The antibiotics include actinomycin D
(dactinomycin), doxorubicin (Adriamycin), bleomycin (Blenoxane), daunorubicin,
plicamycin (Mithracin), mitomycin (Mutamycin), and mitoxantrone (Novantrone).
(See Photo 2.) Among the chemotherapeutic agents,
those most likely to cause stomatitis are the antimetabolites and antineoplastic
antibiotics. The antimetabolites include cyclophosphamide (Cytoxan), cytosine
arabinoside (Ara-C), 5-fluorouracil (5-FU), floxuridine, 6-mercaptopurine
(6-MP), methotrexate, and 6-thioguanine. The antibiotics include actinomycin D
(dactinomycin), doxorubicin (Adriamycin), bleomycin (Blenoxane), daunorubicin,
plicamycin (Mithracin), mitomycin (Mutamycin), and mitoxantrone (Novantrone).
(See Photo 2.)
Patients receiving BRM therapy also run a significant risk of stomatitis. The
worst offenders are interleukin-2, lymphokine-activated killer cells, tumor
necrosis factor, and the interferons.
With the antimetabolites and antineoplastic antibiotics, expect to see
changes in the oral mucosa 2 to 14 days after therapy begins. With BRM therapy,
stomatitis usually appears 2 to 5 days after therapy begins and continues for 7
to 10 days after it ends. Mild stomatitis is usually accompanied by alterations
in taste, voice, and ability to swallow. As the stomatitis progresses, the
patient is less likely to eat, further compromising his oral cavity.
Bone marrow transplantation, the third common form of cancer treatment, can
produce severe, long-lasting oral cavity complications, including mucositis,
xerostomia, loss of taste, pain, and bleeding. During the first 2 weeks after
transplant, the mouth is usually infected and ulcerated.
Before the transplant, the patient receives high-dose chemotherapy and
full-body radiation, making him vulnerable to oral inflammation and infection.
Within 4 to 14 days after pretreatment begins, he may develop
hyperkeratinization (visible as white patchy areas) as well as erythema,
atrophy, and increased vascularity that will continue during the posttreatment
period.
After the transplant, his vulnerability continues because of
immunosuppressive treatment using methotrexate, plus the possibility of
graft-versus-host disease (GVHD). If GVHD occurs, it usually begins on day 15
through 20 and causes mucosal atrophy, erythema, and xerostomia. If GVHD or
infection doesn't develop, the oral cavity will begin healing at about day 21.
HIV-positive patients. The mouth is particularly vulnerable to the
effects of HIV disease. Oral infections result primarily from the
immunosuppression inherent in the disease. But other oral manifestations are
either idiopathic to acquired immunodeficiency syndrome (AIDS) (directly related
to the AIDS virus or to other syndromes common to AIDS patients) or associated
with opportunistic disorders such as Kaposi's sarcoma and non-Hodgkin's
lymphoma.
Problems that are idiopathic to AIDS include blood-filled purpuric oral
lesions associated with idiopathic thrombocytopenic purpura, salivary gland
enlargement and subsequent xerostomia, and recurrent aphthous oral ulceration.
Photo 3: Kaposi's sarcoma

With Kaposi's sarcoma, lesions frequently appear first in the mouth, usually
on the hard palate. These lesions may be flat or raised and are usually red,
blue, or purple. (See Photo 3.) Kaposi's sarcoma also can cause a pigmented
enlargement of gingival tissues and enlargement of the mucosa without pigmented
changes.
Non-Hodgkin's lymphoma may initially produce a firm, painless swelling
anywhere in the mouth. The lesion may initially be covered by intact mucosa,
which can become ulcerated from irritation or trauma.
Others at risk
Besides the elderly and those with cancer or HIV infection, patients at
special risk for oral problems include those with autoimmune disease, diabetes,
and renal disease.
Autoimmune diseases that affect the epithelium are likely to produce
vesicular or bullous oral lesions that appear as intact or ruptured blisters.
These have an insidious onset, are generally painful, and become chronic. When
the autoimmune disease affects connective tissue, involvement of the parotid
glands can produce xerostomia, increasing the possibility of caries and
periodontal disease.
Patients with scleroderma, such as burn patients with contracting perioral
injury, may develop problems because of difficulty opening their mouths, which
makes mouth care difficult. Finally, lupus erythematosus can produce soft tissue
lesions and white keratotic areas.
Diabetes decreases circulation to the skin and mucous membranes. These
highly vascular tissues are then at risk for inflammation and ischemic
ulceration. Poor healing of these lesions is likely, and the potential for
secondary infection is high.
In patients with renal disease, oral dysfunction can be an ominous
sign that uremia is imminent. Indicators include spontaneous gingival bleeding;
a red, dry mucosa covered by a thick, gray exudate; and multiple small ulcers
located on the buccal mucosa and along the mucocutaneous junction. Other
indicators include xerostomia, ammonia smell on breath, and patient complaints
of a metallic or salty taste.
Problems and interventions
Like other body systems, the mouth is designed to respond to disease and
other insults. At first, it mobilizes defenses to maintain integrity and
function. (See Rating 2 in
Keeping Score: A Numeric Gauge of Your Patient's Oral Health.)
Failing that, it quickly shifts tactics to resist the invasion's impact (Rating
3).
If resistance doesn't succeed--a common outcome with immunosuppressed and
malnourished patients--the oral cavity succumbs (Rating 4). Pain, if it hasn't
already started, sets in; infection and bleeding are probably imminent;
nourishment drops off as eating becomes difficult.
To combat each of these problems, you'll need to have a systematic plan of
care. Let's review the interventions at your disposal. Of course, make sure you
document all your oral care assessments and interventions. Also encourage
your facility to include a systematic approach to oral care as part of its
policies and procedures and to involve a multidisciplinary team of caregivers as
needed. (See Preventing
and Managing Oral Care Problems.)
Managing pain
Pain accompanying inflammation and ulceration can deprive the patient of rest
and sleep, limit his ability to communicate, and reduce his nutritional intake.
It also makes performing oral hygiene more difficult, compounding problems.
For temporary numbing, use topical anesthetics, as ordered--either painted or
sprayed onto the painful areas or swished over the mucosa's surface. Two topical
anesthetics used are dyclonine and benzocaine; they're only minimally absorbed,
so the chance of systemic effects is practically eliminated.
Dyclonine, available in 0.5% and 1% solutions, begins working after about 2
minutes and lasts up to 30 minutes. A preparation of 20% benzocaine in a
water-soluble base--or a benzocaine lozenge--begins working in about 30 seconds
but lasts only 5 to 15 minutes.
Photo 4: Pseudomonas infection
 You might also use viscous
lidocaine because it has a longer duration of action (about 40 minutes). But
it's systemically absorbed and has been associated with cardiac and central
nervous system complications, so avoid using it frequently, especially with
patients who have cardiac problems or seizure disorders. Make sure the patient
isn't allergic to "caine" derivatives before using such anesthetics as lidocaine
and benzocaine. You might also use viscous
lidocaine because it has a longer duration of action (about 40 minutes). But
it's systemically absorbed and has been associated with cardiac and central
nervous system complications, so avoid using it frequently, especially with
patients who have cardiac problems or seizure disorders. Make sure the patient
isn't allergic to "caine" derivatives before using such anesthetics as lidocaine
and benzocaine.
Apply topical anesthetics as needed, but especially just before meals to make
eating easier. Be sure to check for a gag reflex before the patient eats or
drinks anything, and advise him to be careful when biting and eating hot food
because decreased sensation increases the risk of injury.
Other nonsystemic agents that ease oral pain include:
| mixtures that contain a topical anesthetic, diphenhydramine HCl elixir,
and an antacid (substrates of antacids can increase comfort by coating the
oral mucosa)
|
| sucralfate (Carafate), which seems to bind to damaged mucosal surfactant
proteins, forming a protective coating. (Sucralfate isn't commercially
available in suspension; tablets must be dissolved, not crushed, then the
mixture swished and swallowed.)
|
| a medicated gel (Zilactin) that contains benzyl alcohol and forms an
occlusive film over the ulcerated area, with relief lasting up to 6 hours.
|
Photo 5: Gram-negative infection, such as Escherichia coli,
Klebsiella, and Proteus

Systemic analgesics include aspirin, acetaminophen, propoxyphene, and
codeine. Acetaminophen elixir can be swished in the mouth for both local and
systemic effect. Don't use aspirin if platelet levels are less than 150,000/mm3
or are expected to drop.
Administer systemic analgesics 1-1/2 to 2 hours before meals and on a
schedule between meals if pain persists. Severe mucositis may require opioid
narcotics, also administered on a schedule, not just p.r.n. A continuous
infusion of morphine, with or without patient-controlled analgesia, is an option
for severe or long-lasting pain related to mucositis.
Attacking infection
You'll need to obtain a culture to ensure precise diagnosis and treatment for
patients with mucositis or other oral mucosal problems. You'll also need a
complete blood cell count with a white blood cell differential so you can
evaluate the patient's ability to fight infection. An absolute granulocyte count
below 1,000 microliters indicates a significant risk of infection. In this case,
the usual signs of infection, such as a purulent exudate, may not be present.
Infections can be bacterial, fungal, or viral. Let's look at each type more
closely.
Bacterial. Most infections that accompany stomatitis are bacterial,
with streptococcal infections predominating. In immunocompromised patients,
gram-negative organisms such as Pseudomonas, Escherichia coli,
Klebsiella, and Proteus are most common. Ulcers infected with
Pseudomonas organisms appear as necrotic, with a blue-black eschar
surrounded by an erythematous halo. Ulcers infected with E. coli,
Klebsiella, and Proteus are generally raised, creamy to yellow-white,
moist, glistening, and nonpurulent. They appear as a smooth-edged, raised area
on a painful, red, ulcerated mucous membrane. Ulcers infected by gram-positive
organisms, which are rare, appear as dry, round, brownish yellow wartlike
eruptions. (See Photos 4, 5, and 6.)
Photo 6: Gram-positive infection
 Expect to treat bacterial
infections with topical applications of bacitracin, neomycin, or polymyxin B. If
culture studies warrant, you might also use appropriate systemic antibiotics. Expect to treat bacterial
infections with topical applications of bacitracin, neomycin, or polymyxin B. If
culture studies warrant, you might also use appropriate systemic antibiotics.
Fungal. These infections are common in the very young and old,
patients on antibiotic therapy, and immunocompromised or myelosuppressed
patients. The usual culprit is Candida albicans, which produces thrush.
Photo 7: Candida albicans infection

Thrush appears as a white lesion, resembling cottage cheese,
that's easily scraped off. (See Photo 7.) The infection also can produce an
erosive, erythematous lesion or cheilitis at the corners of the mouth.
If the infection becomes systemic, you may need to administer intravenous
antifungal agents. Fortunately, however, most fungal infections respond well to
topical medication. Nystatin is the antifungal agent most often used for the
treatment of moniliasis (common especially in patients with endotracheal tubes).
Unless contraindicated, have the patient swish and swallow the topical
antifungal preparation. Or, you can make ice pops from the suspension or allow a
troche to slowly dissolve in the patient's mouth. Fluconazole (Diflucan) is also
a potent antifungal agent used to treat Candida, especially in patients
with HIV disease. Other antifungal agents include ketoconazole, a systemic
agent, and clotrimazole (Mycelia Troche), a lozenge that must be dissolved
slowly in the mouth.
Photo 8: Herpes simplex infection

Viral. Viral oral infections caused by herpes simplex
virus type 1 usually appear as a cluster of vesicles or punctate ulcerations on
the lips or mucosa, causing extreme pain and gingival inflammation and swelling.
(See Photo 8.) Fever, malaise, myalgia, and lymphadenopathy may also be present.
Among the other viruses that may cause oral infections, the most common are
the Coxsackie viruses and herpes zoster virus. The Coxsackie
viruses cause herpangina, in which the patient, often a child, has viral
symptoms and vesicular lesions in the posterior oropharynx. The lesions
frequently rupture and give way to painful ulcers. Herpes zoster
infection produces a unilateral, often linear strip of painful vesicular lesions
that generally follow the distribution of a branch of the fifth cranial nerve.
In the otherwise healthy patient, care for viral infections should be aimed
at palliation, control of fever, and hydration. In the immunocompromised
patient, you'll need specific antiviral therapy as well as aggressive treatment
to prevent secondary bacterial infection. For antiviral therapy, expect to use
acyclovir (Zovirax), which is available as a topical ointment or in 200-mg
capsules or suspension, or the newer valacyclovir (Valtrex), which is taken
orally in 1-gram doses three times daily for 7 days. Valtrex is contraindicated
in patients with a known hypersensitivity or intolerance to valacyclovir,
acyclovir, or any component of the formulation. In patients who are seropositive
to the herpes simplex virus and at high risk for immunosuppression (for
example, bone marrow transplant patients), prophylactic treatment is
recommended.
Bleeding and malnutrition
In the oral mucosa, bleeding usually occurs when soft, fragile clots form,
break away, and re-form, so the blood oozes out intermittently. To control this,
apply pressure with a piece of gauze saturated with ice water or a wet tea bag
that has been frozen.
Also effective are ice water irrigations, topical thrombin, or a fibrinolysis
inhibitor such as 25% syrup of aminocaproic acid (Amicar). Be careful about
using aminocaproic acid if the patient has thrombocytopenia; even the oral rinse
can precipitate disseminated intravascular coagulation.
When the platelet level is less than 40,000/mm3, bleeding may be
difficult to control; when it's less than 20,000/mm3, the potential
exists for spontaneous bleeding.
As for nutrition, oral dysfunction can wreak havoc on the patient's
nutritional status. Decreased salivation dulls taste perception and inhibits
chewing, swallowing, and digesting. Oral pain makes patients reluctant to eat.
The result is malnutrition, vitamin deficiencies, and dehydration--all of which
intensify mouth problems.
Maintain ongoing evaluations to measure the impact of oral complications on
the patient's nutritional status. Promote healing with a diet that's high in
protein and calories, eaten in multiple small amounts, and supplemented with
vitamins and minerals. Avoid foods that are coarse, rough, acidic, or spicy.
Offer meals that are warm rather than hot. Cold and frozen foods such as ice
pops, ice cream, and frozen yogurt are soothing and refreshing.
Severe mucositis can quickly lead to dehydration and malnutrition. Until
healing occurs, the patient may need total enteral or parenteral nutrition. When
necessary, seek a nutrition consultation when patients are assessed to be at
high risk for malnutrition from oral cavity dysfunction.
Full attention
With sicker patients and hectic schedules, you might be tempted to relegate
oral care to a minor concern. Don't make that mistake. By giving your patient's
oral care full attention, you'll keep him comfortable and promote healing. See
Fact vs. fiction:
Moisturizers, toothpaste, mouthwash, and more.
SELECTED REFERENCES
Erickson, L.: "Oral Health Promotion and Prevention for Older Adults,"
Dental Clinics of North America. 41(4):727-50, October 1997.
Jackonen, S.: "Dehydration and Hydration in the Terminally Ill: Care
Considerations," Nursing Forum. 32(3):5-13, July 1997.
Meraw, S. and Reeve, C.: "Dental Considerations and Treatment of the Oncology
Patient Receiving Radiation Therapy," Journal of the American Dental
Association: JADA. 129(2):201-205, February, 1998.
Mojon, P., et al.: "Oral Health and History of Respiratory Tract Infection in
Frail Institutionalised Elders," Gerodontology. 14(1):9-16, July 1997.
This offering may not be reproduced without the permission of Sage Products
Inc. and The Nursing Institute. © March 1999 Sage Products Inc. and Springhouse
Corporation a member of the Reed Elsevier plc group, 1111 Bethlehem Pike, P.O.
Box 908, Springhouse, PA 19477.
PROVIDER INFORMATION:
The Nursing Institute is an affiliate of Springhouse Corporation,
publisher of Nursing99. The Institute is accredited as a provider of
continuing education (CE) in nursing by the American Nurses Credentialing
Center's Commission on Accreditation and by the AACN. This test qualifies for
AACN CERP category A. The Nursing Institute is also an approved provider of CE
in states where it is mandatory for license renewal.* Your Nursing
Institute–issued CE contact hours are valid wherever you reside.
*Provider numbers: Alabama, ABNP0210; California, 5264; Florida, FBN2424; and
Iowa, 136 (Category 1), Texas (Type 1), AACN 8227.
Any commercial product presented or displayed within the educational
activity is not indicative of endorsement or approval by The Institute.
 forma acestei
pagini nu a fost inca definitivata forma acestei
pagini nu a fost inca definitivata |