Pneumocystis Pneumonia
Pneumocystis jirovecii
What is pneumocystis?
A form of pneumonia, caused by the yeast-like fungus (which had previously been erroneously classified as a protozoan) Pneumocystis jirovecii. Pneumothorax is a well-known complication of PCP. An acute history of chest pain with breathlessness and diminished breath sounds is typical of pneumothorax.
Pneumocystis jirovecii
How the disease been found?
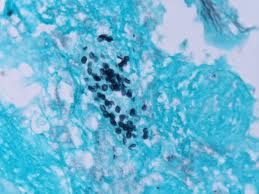
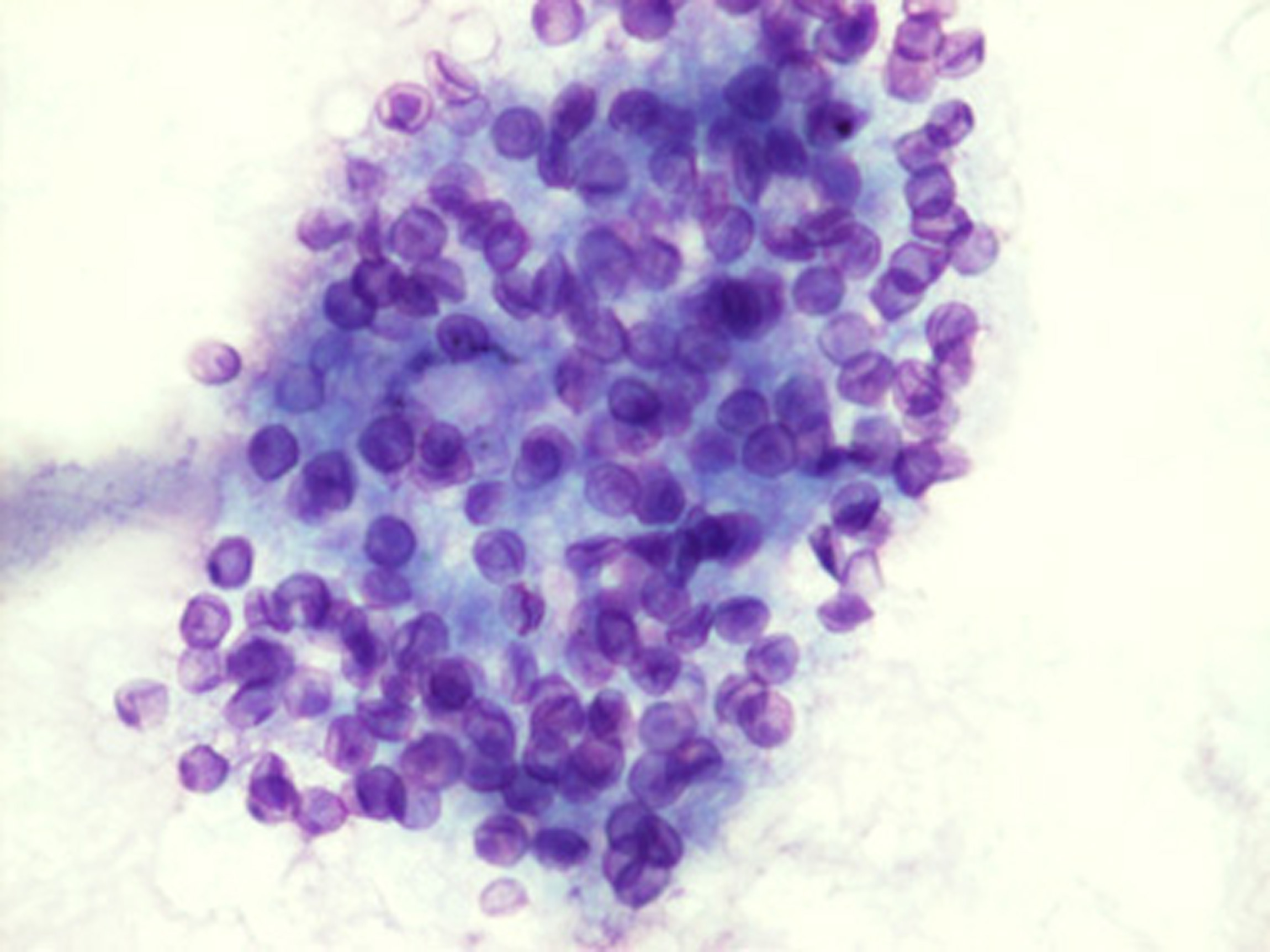
The diagnosis is confirmed by the identification of Pneumocystis jiroveci in induced sputum or bronchoalveolar lavage (BAL) material (washings of the respiratory tree). In situations where these two techniques cannot be used, transbronchial biopsy or open lung biopsy may prove necessary. In addition, immunofluorescence microscopy using monoclonal antibodies can identify the organisms with higher sensitivity than conventional microscopy.
Pnemocystis cycle
Symptoms
-
Fever,
-
Non-productive cough (because sputum is too viscous to become productive),
-
Shortness of breath (especially on exertion),
-
Weight loss,
-
Night sweats.
There is usually not a large amount of sputum with PCP unless the patient has an additional bacterial infection. The fungus can invade other visceral organs (such as the liver, spleen, and kidney), but only in a minority of cases. Common symptoms of pneumocystis pneumonia include the subtle onset of progressive dyspnea, and low-grade fever. Acute dyspnea with pleuritic chest pain may indicate the development of a pneumothorax. Physical examination typically reveals tachypnea, tachycardia, and normal findings on lung auscultation
How can we cure?
-
Trimethoprim–sulfamethoxazole
most effective in treating severe pneumocystis pneumonia. Unfortunately, adverse effects are common, and patients with known allergies to sulfa cannot tolerate this therapy. Patients without AIDS but with severe pneumocystis pneumonia, a dose of 60 mg or more of prednisone daily resulted in a better outcome than lower doses of prednisone.13
2. Antipneumocystic medication
is used with concomitant steroids in order to avoid inflammation, which causes an exacerbation of symptoms about four days after treatment begins if steroids are not used. Most commonly used medication is trimethoprim-sulfamethoxazole, but some patients are unable to tolerate this treatment due to allergies. Other medications that are used, alone or in combination, include pentamidine, trimetrexate, dapsone, atovaquone, primaquine, pafuramidine maleate (under investigation), and clindamycin. Treatment is usually for a period of about 21 days.
is less often used as its major limitation is the high frequency of side effects. These include acute pancreatitis, renal failure, hepatotoxicity, leukopenia, rash, fever, and hypoglycaemia.Primary prophylaxis against pneumocystis pneumonia in HIV-infected adults, including pregnant women and patients receiving HAART, should begin when the CD4+ count is less than 200 cells per millimeter or if there is a history of oropharyngeal candidiasis.8 Medications recommended for prophylaxis are listed in Table 1Table 1Drugs for Prophylaxis against Pneumocystis Pneumonia.. Patients who have had previous episodes of pneumocystis pneumonia should receive lifelong secondary prophylaxis, unless reconstitution of the immune system occurs as a result of HAART. Primary or secondary prophylaxis should be discontinued in HIV-infected patients who have had a response to HAART, as shown by an increase in the CD4+ cell count to more than 200 cells per cubic millimeter for a period of three months. Prophylaxis should be reintroduced if the CD4+ count falls to less than 200 cells per cubic millimeter.
How to heal people without HIV?
Immunosuppressive medications
who have an underlying acquired or inherited immunodeficiency should receive prophylaxis against pneumocystis pneumonia. In a retrospective series, a corticosteroid dose that was the equivalent of 16 mg of prednisone or more for a period of eight weeks was associated with a significant risk of pneumocystis pneumonia in patients who did not have AIDS.
How to treat people with cancer?
Similar observations have been noted in patients with cancer or with connective-tissue disease that was treated with corticosteroids.
The notion that trimethoprim–sulfamethoxazole is contraindicated for pneumocystis pneumonia prophylaxis in patients treated with methotrexate may be outdated, because in patients treated with up to 25 mg of methotrexate per week who received prophylaxis, severe myelosuppression did not develop.
Such patients need to receive folate supplementation (1 mg per day), or leucovorin on the day after receiving methotrexate, and careful monitoring of the results of complete blood counts and liver-function tests is necessary.