Modified Estimation of Occupational Effective Dose Applied
to Angiocardiography Procedures in Jordan
By M. S. AL-ARIF and A.M.Shamoun.
Abstract:
Described is a modified method to estimate the occupational effective
dose in the field of angiocardiography examinations. This method uses thermoluminescent
dosimeter (TLD) badges fixed over and under protective lead aprons. Used
are appropriate correction factors for dose build-up at regions of high
exposure with appropriate weighting factors. The derived result is 7.28
times higher than that stated in the previous method,(1) which
is above the accepted limit.
Introduction
During angiocardiography examinations workers are subject to higher
dose levels than in any other x-ray examination due to the close proximity
to the x-ray machine. An apron protects most of the body except the head,
neck and extremities. Many attempts (l-7) were made to estimate
the effective dose in Fluoroscopy examinations which were summarized by
Al-Shakhrah et.al (1) .In their attempt to estimate the effective
dose in angiocardiography examinations in Jordan, the authors used the
weighting factor for remainder tissues defined by the ICRP(4) as
representative of the weighting factor for the extremities. No correction
factor for the proximity of the extremities to the source of irradiation
during examination was considered. The authors collected thermoluminescent
dosimeter (TLD) data from the Royal Jordanian Scientific Society for 235
workers over a period of 12 months. This data was used in the calculation
of effective dose according to the present modified equation.
Present Method
The consequences following an absorbed dose depend on the magnitude of the dose, the type and energy of the radiation, and the distribution of the dose within the body (4).
Parts of a worker's forearm are subjected to high exposures due to the proximity to the source of radiation during examination processes. Therefore, it is assumed the forearm is divided into two areas. The first area represents the hand (with the extremities), which is situated at an average distance of about 5 cm or less from x-ray source. The second area represents the rest of the forearm, which is situated at an average distance of about 25 cm from the x-ray source. These areas are subjected to higher doses than that recorded by the TLD on the trunk due to their proximity to the x-ray source. Therefore, each area must be multiplied by a suitable correction factor, referred to as, the dose build-up factor "B" which represent the dose gradient at any distance from the source compared to the dose at the position of the TLD on the trunk. In addition, the extremities were included in the remainder organ category and given a weighting factor of 0.025).(1)
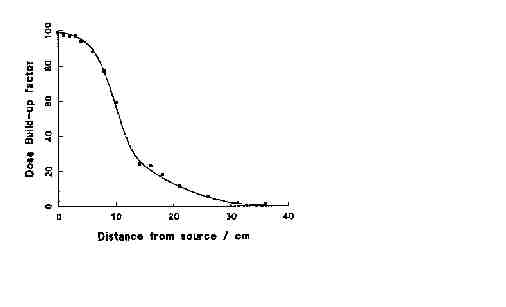
To determine the dose build-up factor "B" at any distance from the source, the fluence rate from a 30-kVp x-ray machine was measured with a G-M tube, and the dose build-up factor is derived from Figure 1.
The following dose build-up factors, B. were assigned for each selected area of the forearm as follows:
1 For the hand (at 5 cm from the source), B5 = 90.
2 For the rest of the arm (at 25 cm from the source), B25=
6.
Modified Method
The skin weighting factor (w=0.01) was used to represent the weighting
factor for the extremities and the rest of the forearm as opposed to the
remainder category. Dose to the remainder organs is taken to be the average
dose to the adrenals, brain, small intestine, kidney, muscle, pancreas,
spleen, thymus, upper large intestine, and uterus.(4) This average
dose is weighted by a factor of 0.05. If one of the above organs included
in the remainder category receives the highest dose, then that organ is
given a weighting factor of 0.025 and the average dose to the other tissues
in the remainder are weighted by a factor of 0.025. It is important to
note the extremities are not one of the remainder tissue organs. Therefore,
they should not be weighted by a factor of 0.025. Since the extremities
are part of the skin they should be weighted by a factor of 0.01.
When all the above modifications were considered, the modified effective
dose equation for fluoroscope examinations in Jordan becomes:
E=Hu+0.05Ho+[0.01xB5xHos+0.01xB25xHos]
Eq. 1
Where:
(Hu) represents the dose under the lead apron
(Ho) represents the total body equivalent dose over the apron
(Hos) represents the skin equivalent dose over apron
Applying the dose build up factors Equation 1 becomes:
E=Hu+0.05Ho+0.96Hos Eq. 2
Result and Discussion
The Royal Jordanian Scientific Society provided each worker with two TLD badges, one to worn over the apron and one worn under the apron over at the same position on the trunk. Each TLD gives information about the deep or organ dose and the shallow or skin .The following values for the average TLD readings where determined by the authors (l) with a standard error of ±2.6 for the effective dose.
Hu = under apron TLD body dose reading = 1.5 mSv
Ho = over apron TLD body dose reading =11.9 mSv
Hos = over apron TLD skin reading = 17.1 mSv.
When these values are inserted into Equation 2 the effective dose becomes;
E = 18.5 ±2.6 mSv. This value for the effective dose is 7.28 times
greater than originally reported by the authors (1) (E=2.54
±2.6 mSv). The value calculated by this revised method may be above
the limit recommended by ICRP-60 (4).
Figure l. The Dose Build-up Factor from the X-ray Source
References
3 I.A.AL-Shakhrah and Y.S.Abu-Khaled, "Determination of Occupational Effective Dose in Angiocardiography in Jordan," Radiation Protection Management, 41-47, March/April 1999.
4 Faulkner, K. and Marshall, N.W., "The Relationship of the Effective Dose to Personnel and Monitor Reading for Simulated Fluoroscopic Irradiation Conditions," Health Phys., 65,502-508,1993.
5 National Council on Radiation Protection and Measurements, Implementation of the Principle of As Low As Reasonable Achievable (ALARA) for Medical and Dental Personnel, NCRP report No. 107, 1990.
6 International Commission on Radiological Protection, 1990, Recommendations of the International Commission on Radiological Protection, Oxford: Pergamon Press; ICRP Publication 60; Ann ICRP 21, 1-25, 1991.
7 Gill, J.R., Beaver, P.F and Dennis, J.A, "The Practical Application of ICRP Recommendations Regarding Dose Equivalent Limits for Workers to Staff in Diagnostic X-ray Departments," 5th International Congress of the International Radiation Protection Association, Book of Papers 1,1518, 1980.
8 Webster, E.W., "EDE for Exposure with Protective Aprons," Health Phys. 56, 568-569, 1989.
9 Niklason, L.T., and Marx, M.V., and Chan Heang-ping, "The Estimation of Occupational Effective Dose in Diagnostic Radiology with Two Dosimeters," Health Phys. 67,611-615, 1994.