PARTURITION BY GWINYAI MASUKUME MBChB II
What is labour? How long does labour last? What are the stages of labour? What triggers labour? What are the signs labour is starting? Positions during second stage of labour? What does the first stage feel like? What does the second stage feel like? What does the third stage feel like? Pain relief? Does support help? Apgar test What is a caesarean? Home births? What is an episiotomy? Calculation of due date? References for section:
What is labour?
<TOP>
Labour
is the process or the effort of childbirth.
Since labour can have complications and differ widely from woman to
woman, focus and reference will be on normal labour.
During labour, the fetus and the placenta (afterbirth) are delivered from the uterus (womb) through the birth canal into the outside world. Labour begins naturally from 37 to 42 completed weeks, dated from the first day of the last normal menstrual period. Before 37 completed weeks the labour is premature and is post-term after 42 completed weeks. Typical labour ends in the cephalic (headfirst) delivery of a live, healthy baby to a healthy mother.
How long does labour last?
<TOP>
Labour generally lasts between 15-16 hours, in a woman's first pregnancy and tends to be shorter (6-8 hours), in subsequent pregnancies. To reiterate, labour can be a lot longer or shorter than the average times .
What are the stages of labour? <TOP>
The effort of labour occurs in three stages. In addition, latent (initial) and active phases divide the first stage into two. However, these are arbitrary distinctions of an otherwise natural and continuous process.
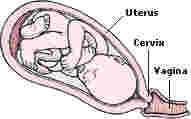
FIRST
STAGE
From
the beginning of labour to the full opening/dilation of the cervix to about 10
centimetres.
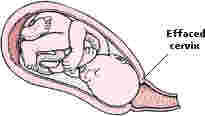
Latent/Initial
Phase
Contractions become progressively stronger and more rhythmic. Discomfort is minimal. The cervix effaces (thins) and opens to about 4 centimetres. This phase lasts an average of 12 hours in first pregnancy and 5 hours in subsequent pregnancies.
Active
Phase
The cervix opens from about 4 centimetres to the full 10 centimetres. The presenting part of the baby, usually the head, begins to descend into the woman’s pelvis. The woman begins to feel the urge to push as the baby descends. This phase averages about 3 hours in a first pregnancy and 2 hours in subsequent pregnancies.
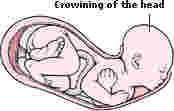
SECOND
STAGE
From the complete opening of the cervix to the delivery of the baby. This stage averages about 45 to 60 minutes in a first pregnancy and 15 to 20 minutes in subsequent pregnancies.

THIRD
STAGE
From delivery of the baby to delivery of the placenta. This stage usually lasts only a few minutes, but may last up to 30 minutes.

What triggers labour? <TOP>
The
mechanisms surrounding childbirth are not completely understood, but it appears
that a hormonal signal from the fetus itself triggers labour.
Current research suggests that several factors are involved in
initiating labour.
Hypotheses of initiation of labour:
Reaching
a threshold level of stretch activates G-proteins of the Rho subfamily which
in turn produce a cascade of events. These
proteins, located in muscle cells of the uterus initiate contraction.
Statistics show that multiple pregnancies usually end prematurely,
presumably due to the high degree of stretching.
Women
with high levels of CRH (corticotrophin releasing hormone) in premature
births and low levels of CRH in post-term births suggest a likely trigger.
Whether the CRH source is maternal or placental, the positive effect
of CRH on substances causing contraction is evident.
Sheep research indicates that oestrogen concentrations rise and progesterone concentrations decline just prior to labour. Whether a shift in the levels of these two hormones is the primary trigger or response is debatable.
What are the signs labour is starting? <TOP>
The
muscular layer of the uterus contracts sporadically during pregnancy and some
women may be aware of the contractions. These "Braxton-Hicks contractions", which intensify toward term are responsible
for false labour and do not signal labour onset.
The appearance of a mucus discharge tinged with blood (the show) from the vagina provides a more certain sign of the onset of labour. "The show", is not usually a cause for concern as it is merely the remains of the mucus plug around the cervix. However, the bloody show may appear as early as three days before contractions begin or even during labour.
Sometimes, the amniochorionic membrane may rupture followed by a sudden gush, then trickle of amniotic fluid from the vagina. Around 80 to 90% of women whose membranes rupture before, but close to their due date go into labour spontaneously within a day. It is therefore important to quickly inform healthcare providers of the rupture commonly referred to as the ‘breaking of the waters’. Sometimes the waters break after labour has started, or may need to be broken by the midwife or doctor.
The onset of regular painful contractions is the most conclusive indicator of labour, though it is difficult to pinpoint their exact start because of the irregular Braxton-Hicks contractions. A typical labour may begin with contractions coming every 10 minutes, lasting thirty seconds each, and gradually increasing to every 3 minutes, lasting forty to sixty seconds each. Uterine contractions are involuntary.
Positions during second stage of labour? <TOP>
Over
the decades, controversy has surrounded whether sitting, squatting, lying or
other positions are suitable during childbirth. Investigation of the aptness of various positions by
randomised controlled trials gave inconclusive results.
Consequently, women should be encouraged to use the most comfortable
position that poses no danger, until further data allows for informed choice.
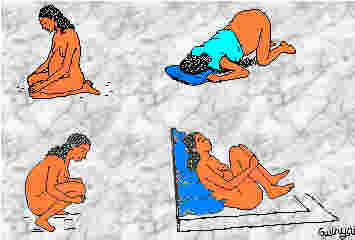
Table 1. Use
of an upright position compared to a horizontal position.
|
Upright
POSITION |
Results |
|
Reduced
duration of second stage of labour |
12
trials - mean 5.4 minutes, 95% confidence interval (CI) 3.9 – 6.9
minutes. |
|
A
reduction in assisted deliveries |
17
trials - odds ratio (OR) 0.82, 95% CI 0.69 - 0.98. |
|
A
reduction in episiotomies |
11
trials - OR 0.73, 95% CI 0.64 - 0.84. |
|
A
smaller increase in second degree perineal tears |
10
trials - OR 1.30, 95% CI 1.09 - 1.54 |
|
Increased
estimated risk of blood loss > 500ml |
10
trials - OR 1.76, 95% CI 1.34 - 3.32 |
|
Reduced
reporting of severe pain during second stage of labour |
1
trial - OR 0.59, 95% CI 0.41 - 0.83. |
|
Fewer
abnormal fetal heart rate patterns |
1
trial - OR 0.31, 95% CI 0.11 - 0.91. |
What does the first stage feel like? <TOP>
During
the latent phase, contractions become more regular, intense and painful.
Nevertheless most women are able to walk about and even talk through
contractions. Meanwhile, it is
important to rest and remain well hydrated in preparation for the time ahead.
Emptying the bladder frequently creates more room for the descent of the
baby.
In
contrast to the latent phase, talking through a contraction will be very
difficult during the active phase. Breathing as well as relaxation techniques and a labour partner can be a great help during this phase. Gentle encouragement
and massage can play an important role as well.
Warm
water quickens labour and reduces pain in the majority of cases.
At this time, pain relief may be administered.
The transition to the second stage is most profound. Symptoms such as shaking, shivering and nausea may be present as contractions peak in intensity and frequency.
What does the second stage feel like? <TOP>
Many women feel an overwhelming urge to push during this stage. Shaking, nausea and a variety of incredible sensations may be present. Most women experience pervading feelings of huge relief and intense euphoria as the baby leaves the body.
What does the third stage feel like? <TOP>
The
mother’s focus will usually have shifted away from the vaginal area to the
baby. Third stage contractions are
relatively mild. A few contractions
may occur after delivery of the placenta if this was the first baby.
Otherwise, intermittent contractions (afterpains) may persist for the
next day or two.
Pain relief? <TOP>
It
is difficult to predict the amount of pain relief required.
Some women cope admirably while others really struggle.
Some pain relief methods:
Entonox
(gas and oxygen):
A mixture of oxygen and nitrous oxide (laughing gas) is inhaled through
the mouth altering pain perception. The
pain relief is good and takes about half a minute to set in.
This mixture is safe for both the mother and baby.
Pethidine:
This potent painkiller is mostly injected, but usually makes the mother
drowsy and crosses the placenta. The
baby may be slow to start breathing and sucking.
However, administration of the antidote naloxone reverses the
effects of pethidine.
Epidural: Injection of a local anaesthetic around the nerves that conduct pain, provides excellent pain relief. A thin tube delivers anaesthetic to the lower back thereby providing constant relief. Delivery of fluid from a drip into an arm vein prevents blood pressure from falling. There is evidence that epidurals prolong the first two stages of labour and cause babies to cry a lot several weeks after birth.
Transcutaneous
electrical nerve stimulation (TENS):
Delivery of a current through four electrodes placed in the lower back
blocks pain conduction. This
method requires a period of acclimatisation and must be practised during
early pregnancy. TENS has no
known adverse effects on the baby, but is ineffective for some women.
Does support help? <TOP>
The
presence and support of a labour partner, usually the father, has been
demonstrated to produce a more favourable outcome. According to a 2001 Cochrane Review "the continuous
presence of a support person reduced the likelihood of medication for pain
relief, operative vaginal delivery, caesarean delivery, and a 5-minute Apgar
score less than 7." Continuous
support was also associated with a slight decrease in the length of labour.
Apgar test <TOP>
A score is given for each sign at one minute and five minutes after the birth (see Table 2). If there are problems with the baby an additional score is given at ten minutes. A score of 7-10 is considered normal, while 4-7 might require some resuscitative measures, and babies with apgars of 3 and below require immediate resuscitation.
Table
2. Apgar
test.
|
|
|
0
Points |
1
point |
2
points |
|
A |
Activity |
Limp |
Some
flexing (bending) of arms and legs |
Active
motion |
|
P |
Pulse |
No
heart rate |
Fewer
than 100 beats per minute |
More
than 100 beats per minute |
|
G |
Grimace |
No
response to airways being suctioned |
Grimace
during suctioning |
Grimace
and cough or sneeze during suctioning |
|
A |
Appearance |
The
baby's whole body is completely blue or pale |
Good
colour in body with blue hands or feet |
Completely
pink or good colour |
|
R |
Respiration |
Not
breathing |
Weak
cry; may sound like whimpering or grunting |
Good,
strong cry |
What is a caesarean? <TOP>
This
is procedure where the doctor makes an incision in the abdomen and uterus and
removes the baby through it. The procedure takes its name from a law passed by the Roman leader Julius Caesar to remove fetuses from dead pregnant women for separate burial.
Some
women are aware that they will need a caesarean, while others may have one
because of complications during labour (see Table 3). Most caesareans are performed with an epidural.
It
is possible to have a vaginal birth after a caesarean (VBAC).
In fact, about 70% of women who try a VBAC succeed.
Horizontal uterine incisions and vertical ones made in the lower section
of the uterus have greatly reduced the chance of uterine rupture.
Table
3.
Some reasons for caesarean sections.
|
Planned
CAESAREAN |
Unplanned
CAESAREAN |
|
The
baby is in a - bottom first - or transverse - sideways - position, or
has a known fetal illness or abnormality. |
The
baby's heart rate becomes irregular, which means that he or she may not
be able to withstand a vaginal delivery. |
|
There
are three or more babies. |
The
umbilical cord is wrapped around the baby's neck, which could be a
choking hazard during a vaginal delivery. |
|
The
mother is having a genital herpes outbreak, which can be passed along to
a baby delivered vaginally. |
The
umbilical cord prolapses, or slips, through the cervix, making it
vulnerable to being compressed during delivery and cutting off the
baby's oxygen supply. |
|
A
mother's pre-eclampsia is rapidly worsening, making it dangerous to
delay delivery. |
The
placenta has abrupted, or torn. |
|
There
is a maternal history of invasive uterine surgery or multiple caesarean
sections. |
The
baby is not moving down the birth canal either because the cervix has
stopped dilating, or for some other reason. |
Home births? <TOP>
Some
women have strong feelings against transforming labour into an unnecessary
clinical process. However, labour
is potentially dangerous for both the mother and child.
Hospitals
can deal better with any emergencies that may arise. Furthermore, it is difficult to predict that a pregnancy and
subsequent delivery are going to be completely risk free.
What is an episiotomy? <TOP>
An
episiotomy is a cut that enlarges the soft tissue outlet as the baby is born.
By estimation, more than 85% of women undergoing a vaginal birth will
sustain some degree of trauma to the region between the thighs (perineum). Of these, 60-70% will require suturing. Whether it is better to perform - under local anaesthetic - an episiotomy which is a straight easily repaired cut or run the risk of a jagged uncontrolled tear remains debatable.
References for section: <TOP>
Beers,
Mark (editor). The Merck Manual of Medical Information - Second Home Edition
[Online]. 2003. Available. http://www.merck.com/mrkshared/mmanual_home2/sec22/ch260/ch260b.jsp.
January 23 2004).
Gupta
JK , Nikodem VC. Position for women during second stage of labour (Cochrane
Review). In: The Cochrane Library, Issue 4, 2003. Chichester, UK: John Wiley
& Sons, Ltd.
Evennett,
K. (1996), Women’s Health an essential guide for the modern woman, Ward
Lock, London pages 107 and 108.
Tommy’s
The Baby Charity. [Online]. 2002. Available. http://www.tommys-campaign.org/website.html.
(January 24 2004).
Vinker,
David. Normal Labour - Childbirth [Online]. 2001. Available. http://www.2womenshealth.co.uk/LABOUR.htm.
(January 22 2004).
World Health Organisation. MCPC-Normal labour [Online]. Unknown. Available. http://www.who.int/reproductive-health/impac/Clinical_Principles/Normal_labour_C57_C76.html. (January 22 2004).
Please note that this information is of a general nature and is meant to assist in improving communication with professionals. The author can be contacted at [email protected]
Last updated 16/06/2004