In vitro fertilisation (IVF)
"in vitro" means "in glass". This refers to the process of in vitro fertilisation which takes place in a glass dish on a laboratory bench. Although this is usually a dish, in the popular mind it was thought to be a test tube — hence the term 'test-tube baby'. Worldwide, thousands of IVF babies have been born since the technique was first used successfully in 1978.

"Naked" Oocyte
History
This technique was developed in the UK by Doctors Patrick Steptoe and Robert Edwards. The first "test-tube baby", Louise Brown, was born as a result on 25th July 1978.
The first in-vitro fertilization in India which produces test-tube baby "Durga" was performed by a Calcutta based doctor Dr. Subhash Mukhopadhay on 3rd October 1978.

The first successful IVF treatment in the USA, producing Elizabeth Carr, took place in 1981 under the direction of Drs Howard and Georgeanna Seegar Jones in Norfolk, Virginia.
Indications
The IVF was developed initially to overcome infertility due to problems of the fallopian tubes, but it was found out that it was successful in most other infertility situations as well.
For IVF to be successful, it requires healthy ova, sperm that can fertilize, and a uterus that can maintain a pregnancy. Most people will only consider to undertake this process when other, less costly reasonable options have failed.
Method
Ovarian stimulation
Treatment cycles are typically started on the third day of menstruation and consist of a regimen of fertility medications to stimulate the development of multiple follicles of the ovaries. In most patients injectable gonadotropins (usually FSH analogues) are used under close monitoring. Such monitoring frequently checks the estradiol level and, by means of gynecologic ultrasonography, follicular growth. Typically approximately 10 days of injections will be necessary. Endogenous ovulation is blocked by the use of GnRH agonists or GnRH antagonists.
When follicular maturation is judged to be adequate, human chorionic gonadotropin (β-hCG) is given. This agent, which acts as an analogue of luteinizing hormone, would cause ovulation about 42 hours after injection, but a retrieval procedure take place just prior to that to recover the egg cells from the ovary. The eggs are retrieved from the patient using a transvaginal technique involving an ultrasound-guided needle piercing the vaginal wall to reach the ovaries. Through this needle follicles can be aspirated, and the follicular fluid is handed to the IVF laboratory to identify ova. The retrieval procedure takes about 20 minutes and is usually done under conscious sedation or general anesthesia.
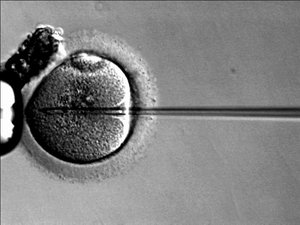
In the laboratory, the identified eggs are stripped of surrounding cells and prepared for fertilization. In the meantime, semen provided by the male partner is prepared for fertilization by removing inactive cells and seminal fluid. The sperm and the egg are incubated together (at a ratio of about 75,000:1) in the culture media for about 18 hours. By that time fertilization should have taken place and the fertilized egg would show two pronuclei. In situations where the sperm count is low a single sperm is injected directly into the egg using intracytoplasmic sperm injection (ICSI). The fertilized egg is passed to a special growth medium and left for about 48 hours until the egg has reached the 6-8 cell stage.
Laboratories have developed grading methods to judge oocyte and embryo quality. Typically, embryos at the 6-8 cells stage are transferred three days after retrieval. In many programs, however, embryos are placed into an extended culture system with a transfer done at the blastocyst stage, especially if many day-3 embryos are available. Blastocysts tend to give higher pregnancy rates.
The embryos judged to be the "best" are transferred to the patient's uterus through a thin, plastic catheter, which passes through her vagina and cervix. Often, several embryos are passed into the uterus to improve chances of implantation and pregnancy.

The patient has to wait two weeks before she returns to the clinic for the pregnancy test. During this time she may receive progesterone - a hormone that keeps the uterus lining thickened and suitable for implantation. Many IVF programs provide additional medications as part of their protocol.
The chances of a successful pregnancy is approximately 20-30 percent for each IVF cycle. There are many factors that determine success rates including the age of the patient, the quality of the eggs and sperm, the duration of the infertility, the health of the uterus, and the medical expertise. It is a common practice for IVF programs to boost the pregnancy rate by placing multiple embryos during embryo transfer. A flip side of this practise is a higher risk of multiple pregnancy, itself associated with obstetric complications.
IVF programs generally publish their pregnancy rates, however comparisons between clinics are difficult as many variables determine outcome. Furthermore, these statistics depend strongly on the type of patients selected.
The major complication of IVF is the development of multiple births. This is directly related to the practice of placing multiple embryos at embryo transfer. Multiple birth are related to increased pregnancy loss, premature labor, obstetrical complications, prematurity, and neonatal morbidity with the potential for long term damage. Strict embryo transfer policies have been enacted to reduce this problem, but are not universally followed or accepted. Spontaneous splitting of embryos in the womb after transfer does occur, but is rare (<1%) and would lead to identical twins. Recent evidence suggest that singleton offspring after IVF is at higher risk for lower birth weight for unknown reasons.
Another major complication, related to the use of ovarian stimulation is the development of the ovarian hyperstimulation syndrome.
If the underlying infertility is related to abnormalities in spermatogenesis, it is plausible, but too early to examine that male offspring is at higher risk for sperm abnormalities.
The issue of birth defects remains a controversial topic in IVF. A majority of studies do not show a significant increase after use of IVF. Some studies suggest higher rates for ICSI , while others do not support this finding . Major birth defect include chromosomal abnormalities, genetic imprinting defects, and multiple organ abnormalities. Hansen et al conducted a systematic review of published studies (including ICSI) and found a 30-40% increase risk of birth defects associated with assisted reproductive technology when compared to children born after spontaneous conception. Possible explanations offered were the underlying cause of the infertility, factors associated with IVF/ICSI, culture conditions, and medications, however, the actual cause is not known.
If multiple embryos are generated, patients may choose to freeze embryos that are not transferred. Those embryos are placed in liquid nitrogen and can be preserved for a long time. The advantage is that patients who fail to conceive may become pregnant using such embryos without having to go through a full IVF cycle. Or, if pregnancy occurred, they could return later for another pregnancy.
Cryopreservation of unfertilized mature oocytes has been sucessfully accomplished, e.g. in women who are likely to lose their ovarian reserve due to undergoing chemotherapy.
Cryopreservation of ovarian tissue is of interest to women who want to preserve their reproductive function beyond the natural limit, or whose reproductive potential is threatened by cancer therapy. Research is trying to address this issue.
Intracytoplasmic sperm injection (ICSI) is a more recent development associated with IVF which allows the sperm to be directly injected in to the egg using micromanipulation. This is used for sperm that have difficulty penetrating the egg and when sperm numbers are very low. ICSI results in success rates equal to IVF fertilization.
Preimplantation genetic diagnosis (PGD) can be performed on embryos prior to the embryo transfer.
Certain ethical issues have been raised from the beginning when IVF was introduced. These concerns include:
The IVF process requires sperm, eggs, and a uterus. To achieve a pregnancy any of these requirements can be provided by a third party (or more parties): third party reproduction. This has created additional ethical and legal concerns. The use of IVF provides also greater range of options for single people and same-sex couples wishing to have children. Although both groups already raise children, IVF facilitates this process. Some people object that this could give psychological problems to the child if they grow up without a mother/father role-model.
A number of cases have achieved notoriety:
While menopause has set a natural barrier to further conception, IVF has allowed women to be pregnant in their fifties and sixties. These women whose uterus has been appropriately prepared receive embryos that originated from an egg of an egg donor. Therefore, their children are not genetically linked to them. Even after menopause the uterus is fully capable to carry out its function. Currently, the oldest woman to give birth is Adriana Iliescu, age 66, from Romania.
While in the United States IVF programs operate under voluntary guidelines, programs in many other countries are subject to regulations that regulate many aspects of IVF practice. In such settings regulations may dictate: