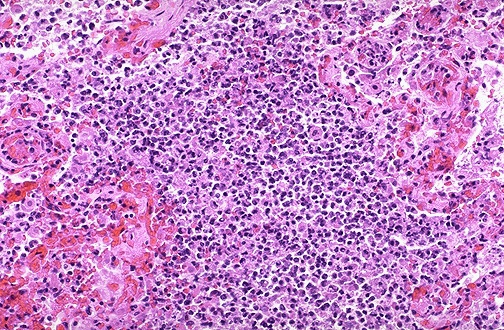
Lung abscess
Click to see other slides: [1] [2]
A
60 yr old alcoholic with poor dentition presented with cough productive of
copious purulent sputum and fever.
1.
What is your diagnosis?
Lung
abscess
2.
List the key histopathological features.
Suppurative
destruction of lung parenchyma
Central area of cavitation filled with pus (neutrophils, necrotic
tissues, inflammatory exudates:
fluid component)
3.
What is the characteristic radiologic finding on chest X-ray?
Air
fluid levels in cavities
Anaerobic abscesses are located in dependent, poorly ventilated and
poorly drained bronchopulmonary segments (lower lobes)
4.
What
are the routes and possible pathogenic mechanism for this type of lung lesions?
Aspiration of infective material
�
Oral
cavity
�
Gastric
contents
Post infection (post-penumonia)
Septic embolism: haematogenous spread
�
Bacterial
endocarditis
�
Thrombophlebitis
Obstruction �
secondary infection (obstruction brought abt by neoplasm, foreign
material)
Others
�
Direct
penetrating injury
�
Spread
of infection from neighbouring organs
�
Haematogenous
seeding of pyogenic bacteria
Primary cryptogenic
5.
Cite
some complications that may result.
Extension
of infection into pleural cavity (empyema)
Purulent pericarditis
Haemorrhage
Septi emboli
�
Brain
abscess
�
Meningitis
Reactive secondary amyloidosis (rarely)
Note: Pulmonary abscesses are usually single and usually occur at the
right lung because the right bronchus is more vertical.
Abscesses caused by bronchiectasis and also pneumonia are frequently
multifocal.
<< PREVIOUS INDEX NEXT SLIDE >>
Copyright � Joseph Ong 2003