Fibrocaseous TB
Click to see other slides: [1] [2] [3] [4]
A
45 yr old woman complained of weight loss, fatigue, fever and night sweats for
several months. She
coughed out blood recently.
1.
What is your diagnosis?
Pulmonary
tuberculosis
3.
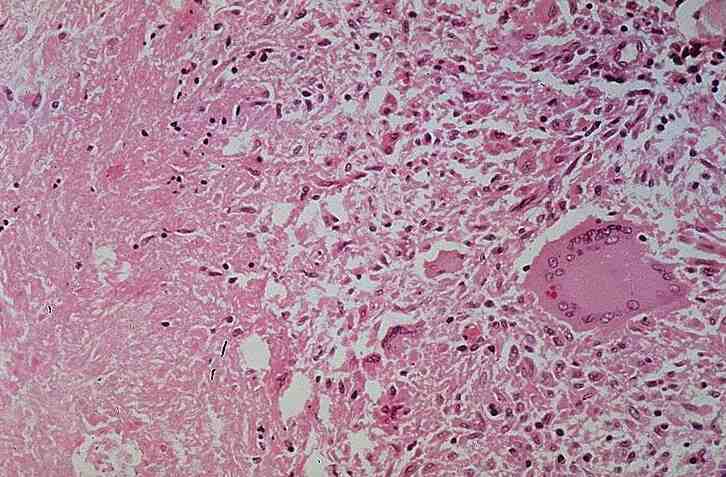
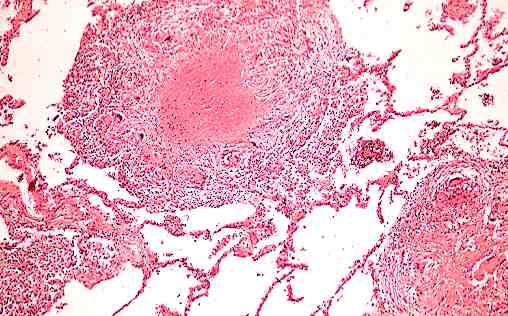
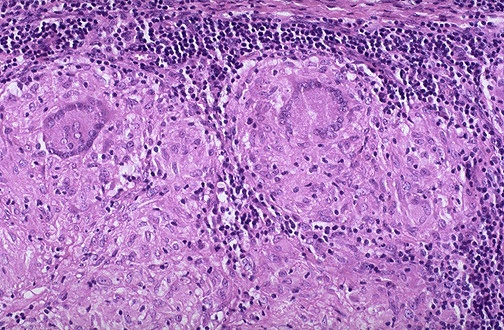
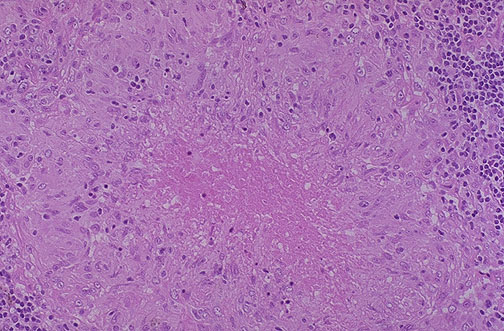
What are the main histological features?
Central
area of caseous necrosis
Surrounded by thick fibrous wall (collagen deposition from fibroblasts)
Giant
cells are hardly visible
Destruction
of lung parenchymal tissue due to chronic granulomatous inflammation with
release of proteases, elastases and other cytotoxic substances by the
macrophages and T cytotoxic cells.
Erosion of tubercle into a vessel leading to hematogenous spread to other organs.
4.
Relate
the haemoptysis to the pathology.
Erosion
of a full patent vessel in the wall of a cavity
Rupture
of a dilated vessel in a cavity (Rasmussen�s aneurysm)
5.
What is the pathogenic mechanism for the necrosis?
CD8+
suppressor T cells lyse macrophages infected with mycobacterium through a
Fas-independent & granule dependent reaction
CD8-4-
(double negative) T cells lyse macrophages through a Fas-dependent reaction
Direct
toxicity of mycobacteria to macrophages
6.
What
is the preferred site for the lesions?
Why?
Apical
parts of the upper lobes (superior segments of lower lobes)
High oxygen tension favours mycobacterial growth (obligate
aerobes)
7.
How
would you confirm your diagnosis?
Smear
of sputum sample / biopsy specimen
Acid
fast bacilli microscopy using Ziehl-Neelson stain
Positive red coloured bacilli should be seen if sample is positive
8.
Where
do you find non-caseating granulomas?
Sarcoidosis.
<< PREVIOUS INDEX NEXT SLIDE >>
Copyright � Joseph Ong 2003
{kind=link}
{kind=link}
{kind=link}