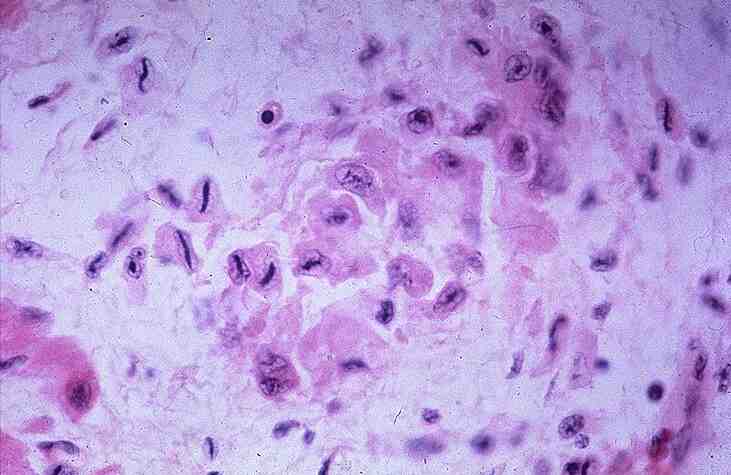
Heart: Rheumatic myocarditis
Click to see other slides: [1] [2] [3]
List
the histopathological features.
Aschoff
bodies: focal but widely disseminated central area of fibrinoid necrosis.
Surrounded
by Anitchow cells (plump macrophages)
-
elongated, condensed chromatin
with spikes
-
caterpillar appearance �
Longitudinal section
-
owl�s eye appearance �
Transverse section
Inflammatory
cells containing lymphocytes and plasma cell.
Multinucleated Aschoff giant cells.
Which
particular part of the heart is affected in this area?
Myocardium:
Interstitial connective tissue between myocardial fibres.
Note: in rheumatic fever, it usually causes pancarditis, that is usually involves all 3 layers of the heart.
What
is the aetiology of this condition?
Streptococcus
pyogenes infection.
Immune mediated inflammatory disease involving a cross reaction between antistreptococcal Ab & tissue glycoproteins.
Would
it be useful to do a Gram stain on the slide?
No. It is a poststreptococcal inflammatory disease, occurring 3 to 5 after the infection.
Rheumatic
fever causes pancarditis.
How would each component of the pancarditis affect cardiac function?
Pericardium�fibrinous
and serofibrinous pericarditis, bread and butter appearance.
�usually
fibrin digested with resolution of exudates in uncomplicated cases.
�complication:
usually
little impairment of cardiac function
Myocardium�myocarditis
�
4 chambers dilated, mural thrombosis�complete
recovery (inflammatory lesions resolution�granulomatous
rheumatoid nodules �
damaging
-
organisation
-
deforming fibrosis
-
commissural fusion �
stenosis
- cusp / leaflet thickening and retraction, shortening and thickening of chordae tendinae leading regurgitation.
What
feature of healing leads to chronic valvular lesions following acute
rheumatic valvular endocarditis?
Fibrosis
Explain
why chronically damaged rheumatic valves are prone to infective
endocarditis?
Damaged heart valves are distorted � roughened surface, leading to calcification and bacterial seeding � abnormal blood flow � turbulence � plaque formation and thrombosis
What
is the significance of asking for history of pharyngitis and joint pain?
One third of all pharyngitis is caused by streptococcal pyogenes, and antibodies
against this bacteria crossreacts with cardiac myocytes causing rheumatic
fever.
<< PREVIOUS INDEX NEXT SLIDE >>
Copyright � Joseph Ong 2003