ENTEROBACTERIACEAE
Outline:
·
Describe the general characteristics of members of the Enterobacteriaceae
family.
·
Identify the normal gut flora and the members that cause opportunistic
infections.
·
Name the common primary intestinal pathogens and their associated
infections.
·
Discuss the laboratory tests used for diagnosis.
1.
Introduction
a.
The Enterobacteriaceae form a large family of gram-negative rods found
primarily in the colon of humans and other animals, many as part of the normal
flora.
b.
They are the major facultative anaerobes in the large intestine but are
present in relatively small numbers compared with anaerobes such as Bacteroides.
c.
Common characteristics:
i.
they are all facultative anaerobes.
ii.
they all ferment glucose.
iii.
none have cytochrome oxidase (i.e., they are oxidase-negative).
iv.
they reduce nitrates to nitrites as part of their energy-generating
processes.
v.
most possess flagella and are motile.
d.
These characteristics are used to distinguish the Enterobacteriaceae from
the nonfermenting gram-negative rods, Pseudomonas aeruginosa, a
significant cause of urinary tract infections and sepsis in hospitalized
patients.
e.
Categories of Enterobacteriaceae and their
representative disease:
|
Source
of site of infection |
Genus |
Representative
disease |
Fermentation |
|
Both
within and outside |
Escherichia |
Urinary
tract infection Traveler’s
diarrhea Neonatal
meningitis |
Occurs |
|
Salmonella |
Typhoid
fever Enterocolitis |
Does
not occur |
|
|
Primarily
within |
Shigella |
Dysentery |
Does
not occur |
|
Vibrio |
Cholera |
Occurs
slowly |
|
|
Campylobacter |
|
|
|
|
Helicobacter |
|
|
|
|
Outside
only |
Klebsiella |
Pneumonia Urinary
tract infection |
|
|
|
Enterobacter |
Pneumonia Urinary
tract infection |
|
|
|
Serratia |
Pneumonia Urinary
tract infection |
|
|
|
Proteus |
Urinary
tract infection |
|
|
|
Pseudomonas |
|
|
|
|
Bacteriodes |
|
|
a. The bacterial inhabitants of the human gastrointestinal tract constitute a complex ecosystem.
b. More than 400 bacterial species have been identified in the feces of a single person; anaerobic bacteria predominate.
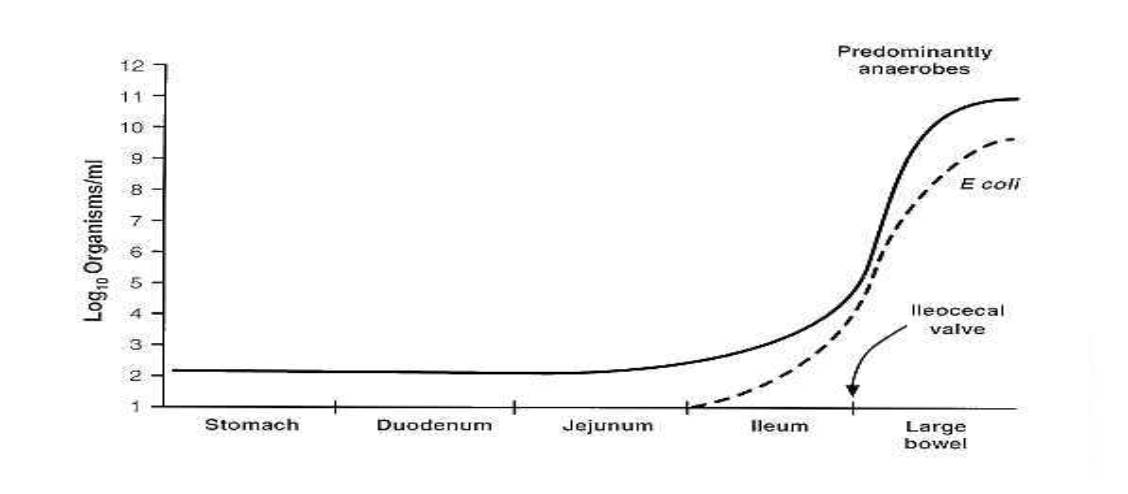
c. The upper gastrointestinal tract (the stomach, duodenum, jejunum, and upper ileum) normally contains a sparse microflora; the bacterial concentrations is less than 104 organisms/ml of intestinal secretions.
d. Most of these organisms are derived from the oropharynx and pass through the gut with each meal.
e. Colonization of the upper intestine by coliform organisms is an abnormal event and is characteristic of certain infectious pathogens such as Vibrio cholerae and enterotoxigenic Escherichia coli.
f. In contrast, the large intestine normally contains a luxuriant microflora with total concentrations of 1011 bacteria/g of stool.
g. Anaerobes such as Bacteroides, anaerobic streptococci, and clostridia outnumber facultative anaerobes such as E coli by a factor of 1,000.
g. Concentration of the bacterial flora in regions of the gastrointestinal tract:
h. The character of the bacterial flora changes not only along the length of the gastrointestinal tract but also cross-sectionally with regard to the mucosal surface. Bacteria occupy the lumen, overlie the epithelial cells, and adhere to the mucosa.
I. Penetration of bacteria through the mucosal surface is an abnormal event; pathogens such as Shigella, Salmonella, and Campylobacter invade in this way.
j. Protective mechanisms of the Gastrointestinal tract:
i. the same mechanisms that control the normal flora also protect the bowel from invasion by pathogens.
ii. gastric acid in the stomach kills most organisms that are swallowed. Individuals with reduced or absent gastric acid have a high incidence of bacterial colonization in the upper small bowel and are more susceptible to bacterial diarrheal disease.
iii. bile has antibacterial properties and thus may be another factor in controlling the flora. Forward propulsive motility (peristalsis) is a key element in suppressing the flora of the upper bowel.
iv. finally, the microflora itself, by producing its own antibacterial substances (e.g., bacteriocins and fatty acids), stabilizes the normal populations and prevents implantation of pathogens.
a. The metabolic capacities of the intestinal bacteria are extremely diverse - bacterial enzymes can use as substrate virtually any compound in the intestinal lumen, whether taken orally or entering the intestine by secretion through the biliary tract or directly across the mucosa.
i. enzymes produced by intestinal bacteria play a central role in the enterohepatic circulation.
ii. substances that undergo enterohepatic circulation are metabolized in the liver, excreted in the bile, and passed into the intestinal lumen, where they are reabsorbed across the intestinal mucosa and returned to the liver via the portal circulation.
iii. the enterohepatic circulation generally involves compounds that are conjugated in the liver to a polar group such as glucuronic acid, sulfate, taurine, glycine, or glutathione.
iv. conjugation increases the solubility of the metabolite in bile, but the conjugated compounds are poorly absorbed by the intestinal mucosa.
v. enzymes produced by intestinal bacteriasuch as ß-glucuronidase, sulfatase, and various glycosidasesdeconjugate these compounds, releasing the parent compounds which are readily absorbed across the intestinal wall.
vi. many endogenous compounds undergo enterohepatic circulation, including bilirubin, bile acids, cholesterol, estrogens, and metabolites of vitamin D.
vii. in addition, many drugs that are excreted by the liver, including digitalis, diethylstilbestrol, morphine, colchicine, rifampin, and chloramphenicol, enter this pathway.
c. Effects of Antibiotics:
i. antibiotics block the enterohepatic circulation by suppressing the intestinal flora and thereby reducing the levels of deconjugating enzymes.
ii. if an antibiotic is given to a patient who is also taking a drug that undergoes enterohepatic circulation, the resulting depression of the enterohepatic circulation will increase the fecal excretion of the drug and thereby lower its plasma level and half life.
iii. for example, the blood levels and half life of the estrogen in birth control pills decrease when antibiotics are administered.
i. enzymes produced by intestinal bacteria are important in the metabolism of several vitamins.
ii. the intestinal microflora synthesizes vitamin K, which is a necessary cofactor in the production of prothrombin and other blood clotting factors.
iii. treatment with antibiotics, particularly in individuals eating a diet low in vitamin K, can result in low plasma prothrombin levels and a tendency to bleed.
iv. intestinal bacteria also synthesize biotin, vitamin B12, folic acid, and thiamine.
v. the intestinal flora is capable of fermenting indigestible carbohydrates (dietary fiber) to short-chain fatty acids such as acetate, propionate, and butyrate.
vi. the major source of such fermentable carbohydrate in the human colon is plant cell wall polysaccharides such as pectins, cellulose, and hemicellulose.
vi. the acids produced from these fiber substrates by bacteria can be an important energy source for the host.
vii. some people are deficient in intestinal lactase, the mucosal enzyme responsible for hydrolyzing the disaccharide lactose in milk.
vii. in these individuals, lactose is not adequately digested and absorbed in the intestine. Lactose that reaches the large bowel undergoes vigorous bacterial fermentation. The result can be distention, flatus, and diarrhea.
a. Like other complex ecosystems, the intestinal microflora is relatively stable over time, maintaining roughly constant numbers and types of bacteria in each area of the bowel.
b. The stability of normal flora both discourages infection by exogenous pathogens and prevents overgrowth of potentially pathogenic members.
c. New organisms that enter the system in contaminated food or water generally are suppressed by the established flora.
d. This suppression is related to production by members of the resident flora of antimicrobial substances such as bacteriocins or short-chain fatty acids, which inhibit the growth of alien microorganisms.
e. Antibiotics that kill off part of the intestinal flora can upset its balance and may open the door to infection or pathologic overgrowth.
a. The normal intestinal flora includes small populations of organisms that cause disease if they overgrow; for example, overgrowth of Clostridium difficile produces severe inflammation of the colon with diarrhea (pseudomembranous colitis).
b. Administration of antibiotics initiates the process by suppressing the normal flora.
i. bacteria from the intestinal flora are the prime cause of infection in the peritoneal cavity when the normal barriers of the intestinal wall are violated.
ii. the intestinal wall can be perforated by trauma (knife wounds, gunshot wounds, blunt trauma), by disease (appendicitis, penetrating intestinal cancers), or by surgical procedures.
iii. once the mucosal barrier is breached, bacteria penetrate through the intestinal wall into the normally sterile peritoneal cavity and its surrounding structures.
iv. poor circulation, reduced oxygen supply, and dead tissue in the vicinity of the perforation promote the formation of an abscess and particularly favor the growth of anaerobic bacteria.
v. cultures of a peritoneal abscess generally yield several types of bacteria from the intestinal microflora, particularly species of Bacteroides, Clostridium, and Peptostreptococcus and E coli.
i. Several enterotoxin-producing bacteria cause diarrheal diseases.
ii. The diarrheal disease caused by Vibrio cholerae and enterotoxigenic strains of E coli has three main characteristics.
iii. First, there is intestinal fluid loss that is related to the action of an enterotoxin on the small bowel epithelial cells.
iv. Second, the organism itself does not invade the mucosal surface; rather, it colonizes the upper small bowel, adhering to the epithelial cells and elaborating the enterotoxin.
v. The mucosal architecture remains intact with no evidence of cellular destruction. and bacteremia does not occur.
vi. Third, the fecal effluent is watery and often voluminous, so that the diarrhea can result in clinical dehydration.
vii. The fluid originates in the upper small bowel. where the enterotoxin is most active.
i. the paradigm of the enterotoxigenic diarrheal diseases is cholera in which stool volume can exceed 1 L/h, with daily fecal outputs of 15 to 20 L if the patient is kept hydrated.
ii. cholera is caused by V cholerae, which is usually ingested in contaminated water.
iii. vibrios that survive passage through the stomach colonize the surface of the small intestine, proliferate, and elaborate the enterotoxin.
iv. cholera toxin acts via adenylate cyclase to stimulate secretion of water and electrolytes from the epithelial cells into the lumen of the gut.
v. the duodenum and upper jejunum are more sensitive to the toxin than the ileum is; the colon is relatively insensitive to the toxin and may still absorb water and electrolytes normally.
vi. cholera stool is described as resembling rice water clear fluid flecked with mucus and is isotonic with plasma.
vii. microscopy reveals no inflammatory cells in the fecal effluent; all that can be seen are small numbers of shed mucosal cells.
i. certain strains of E coli cause diarrheal disease by elaborating enterotoxins.
ii. these strains produce two types of enterotoxin.
iii. one, called heat-labile toxin, is similar in structure and in its mechanism of action to cholera toxin.
iv. the other, called heat-stable toxin, appears to act via guanylate cyclase.
v. Enterotoxigenic E coli strains are the most common cause of travelers' diarrhea.
i. Many strains of Shigella produce an enterotoxin, called Shiga toxin, that causes secretion of fluid from the small intestine.
ii. Shiga toxin has a destructive, cytotoxic effect on the small-bowel epithelium, causing gross injury to the bowel surface; it does not activate adenylate cyclase.
iii. E coli 0157:H7, the organism associated with consumption of undercooked chopped meat, also produces a Shiga-like toxin; it causes bloody diarrhea and colitis.
iv. An organism that produces a different type of cytotoxin is Vibrio parahaemolyticus, a bacterium associated with seafood.
v. Food-poisoning strains of Staphylococcus aureus and Clostridium perfringens both produce enterotoxins that are cytotoxic; the staphylococcal enterotoxin also has a direct effect on the vomiting center in the brain.
a. Unlike the enterotoxigenic organisms, invasive bacteria exert their main impact on the host by causing gross destruction of the epithelial architecture; histologic findings include mucosal ulceration and an inflammatory reaction in the lamina propria.
b. The principal pathogens in this group are Salmonella, Shigella, Campylobacter, invasive E coli, and Yersinia.
i. Salmonella species are a common cause of food poisoning.
ii. the main site of attack is the lower ileum, where the salmonellae cause mucosal ulceration.
iii. they rapidly make their way through the epithelial surface into the lamina propria and enter the lymphatics and bloodstream.
iv. at least two virulence factors are associated with intestinal infection: one responsible for mucosal invasion, and the other causing secretion of fluid and electrolytes into the bowel.
i. Shigella organisms cause bacillary dysentery, an invasive diarrheal disease of the lower bowel in which the stool contains an inflammatory exudate composed of polymorphonuclear leukocytes.
ii. the bacilli invade the epithelium of the colon and cause superficial ulceration.
iii. this invasive process depends on the presence of two virulence factors.
iv. the first mediates the initial penetration of the mucosal surface by destroying the brush border; the bacteria are subsequently engulfed by invagination of the plasma membrane.
v. the second virulence factor allows the organism to multiply within the mucosal tissue.
v. mucosal ulceration results, accompanied by an intense inflammatory response in the lamina propria.
vi. the infection is usually restricted to the mucosa; lymph node involvement and bacteremia are uncommon.
a. The mechanism(s) by which the fluid that causes watery diarrhea is produced in the invasive diarrheal diseases is under debate.
b. Three mechanisms have been proposed.
c. First, Shigella and possibly Salmonella strains apparently produce an enterotoxin that stimulates the mucosa to secrete water and electrolytes.
d. Second, there is evidence that invasive organisms stimulate prostaglandin synthesis at the site of inflammation and that the prostaglandins induce fluid secretion.
e. In experimental animals, fluid secretion can be blocked by prostaglandin inhibitors such as indomethacin and aspirin.
f. Third, some evidence suggests that damage to the colonic epithelium causes diarrhea by prevention of normal resorption of fluid.
9.
Antigens
a.
The antigens of several Enterobacteriaceae, especially Salmonella and
Shigella, are important as they are used for identification purposes,
both in the clinical laboratory and in epidemiologic investigations.
b.
Cell wall antigen:
i.
also known as the O antigen, it is the outer polysaccharide portion of
the lipopolysaccharide.
ii.
the O antigen is the basis for the serologic typing of many enteric rods.
iii.
the number of different O antigens is very large; there are about 1500
types of Salmonella and 150 types of E.coli.
c.
H antigen:
i.
the H antigen is the flagellar protein.
ii.
only flagellated organisms, such as Escherichia and Salmonella,
have H antigens, whereas the nonmotile ones, such as Klebsiella and Shigella,
do not.
iii.
the H antigens of certain Salmonella species can reversibly
alternate between 2 types of H antigens.
iv.
the organisms may use this change in antigenicity to evade the immune
response.
d.
K polysaccharide:
i.
the capsular or K polysaccharide antigen is prominent in heavily
encapsulated organisms such as Klebsiella.
ii.
the K antigen is identified by the quellung reaction in the presence of
specific antisera and is used to serotype E coli and Salmonella typhi.
10.
Laboratory Diagnosis
a.
Specimens suspected of containing members of the Enterobacteriaceae and
related organisms are usually inoculated onto 2 media, a blood agar plate and a
selective differential medium such as MacConkey’s agar or eosin-methylene blue
(EMB) agar.
b.
The differential ability of these latter media is based on lactose
fermentation, which is the most important metabolic criterion used in the
identification of these organisms.
c.
On these media, the nonlactose fermenters, e.g., Salmonella and Shigella,
form colorless colonies, whereas the lactose fermenters form colored colonies.
d.
The selective effect of the media in suppressing unwanted gram-positive
organisms is exerted by bile salts or bacteriostatic dyes in the agar.
e.
An additional set of screening tests, consisting of the triple sugar iron
(TSI) agar and urea agar, is done prior to the definitive identification
procedures.
f.
Urea agar:
i.
the important components of this medium are urea and the pH indicator
phenol red.
ii.
if the organism produces urease, the urea is hydrolyzed to ammonia and
carbon dioxide.
iii.
ammonia turns the medium alkaline, and the color of the phenol red
changes from light orange to reddish purple.
iv.
the important organisms that are urease-positive are Proteus species
and K pneumoniae.
g.
Motility:
i.
Proteus species are very motile and characteristically swarm over
the blood agar plate, obscuring the colonies of other organisms.
ii.
motility is an important diagnostic criterion in the differentiation of Enterobacter
cloacae, which is motile, from Klebsiella penumoniae, which is
nonmotile.
h.
If the results of the screening tests suggest the presence of a Salmonella
or Shigella strain, an agglutination test can be used to identify the
genus of the organism and to determine whether it is a member of group A, B, C,
or D.
11.
The Enterobacteriaceae: important causes of
hospital-acquired infections
a.
Operation on the gastrointestinal tract will release bacteria including
this group and wound infection, peritonitis and abdominal/pelvic abscesses may
result; often these are mixed infections with obligate anaerobes also present.
b.
Hospitalized patients, particularly the sicker and long-term ones, become
widely colonized with coliform organisms, the normal flora at many sites
including the mouth and throat, and skin, becomes partially replaced.
c.
This is partly the result of broad-spectrum antibiotic prescription,
which also favors the survival of resistant strains of these bacteria.
d.
Klebsiella species are important but any of the coliforms can do
this; as well as E. coli and Proteus species, many other members
of the Enterobacteriaceae including Enterobacter, Citrobacter, Morganella and
Providencia species cause nosocomial infections.
e. Infections of the urinary tract, wound site, and lungs are common; invasion of the bloodstream with septicaemia may occur, and these infections can be fatal.
12.
Treatment of infections caused by
Enterobacteriaceae
a.
Ampicillin was the first penicillin derivative with activity against
these bacteria; however many strains now produce one of a variety of beta
lactamase enzymes which destroy the drug and make them resistant.
b.
Amoxycillin is a very similar drug.
c.
Newer injectable cephalosporin antibiotics such as cefuroxime and
cefotaxime are resistant to many of these beta lactamases and are now widely
used in hospital practice.
d.
Unfortunately, the bacteria have responded by producing a new generation
of extended spectrum beta lactamases which also destroy these cephalosporins.
e.
The aminoglycosides like gentamicin kill coliforms rapidly and resistance
is not too common, but they have toxicity problems.
f.
New quinolone drugs like ciprofloxacin were initially useful but again
resistance is emerging rapidly.
g.
For very resistant strains it may be necessary to use one of the penem
antibiotics like imipenem.
h.
Most cases of infectious diarrhea do not require antibiotic treatment:
this should be restricted to patients with more severe disease.