Flagging for Ticks
Contents of this brochure are a result of collaborative efforts of the Lyme Disease Association of Ohio (LDAOhio) and the Ohio Health Department, Vector-Borne Disease Unit.
Any tick can carry and potentially transmit disease. Certain species of ticks can carry and transmit Lyme disease as well as Human Monocytic Ehrlichiosis, Human Granulocytic Ehrlichiosis, Rocky Mountain Spotted Fever, Babesiosis and Tularemia.
Awareness is the first step to prevention of these diseases. Knowing the enemy is your best defense.
Spring and fall are the best time of year to flag for ticks.
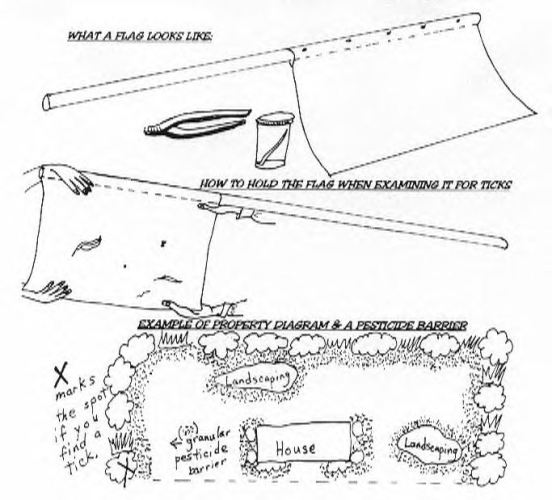
TOOLS I WILL NEED TO FLAG FOR TICKS
HOW DO YOU FLAG A YARD?
WHAT INFORMATION WILL BE ON THE REPORT?
You will be notified about the species of the tick and any test
results concerning disease
WHAT IF A TICK IS INFECTED?
If the
report shows that a tick is infected, do not panic.
Ticks drop off of
birds as well as deer and small rodents.
HOW CAN I PROTECT MYSELF AND MY FAMILY?
You can protect your family and your yard by going to a
lawn and garden store and purchasing a granular pesticide. Most formulas for
turf pests will be effective. Placing a path of the granular pesticide makes a
barrier between the wild and your yard. (see the illustration below) Consider
flagging again to keep the ticks in check.
Call the Vector-Borne Disease Unit if you have any
questions: 614-752-1029
http://www.odh.state.oh.us/ODHPrograms/ZOODIS/VBDP/Pubs/OVN0404.pdf
TICK TESTING AND IDENTIFICATION PROGRAM FORM
Lab Use VDBU No.______________ Vector-borne Disease Unit
Only: Date Rec._____________ 900 Freeway Dr., N.
ID____________________ Columbus, OH 43229
Results_______________ 614-752-1029
INSTRUCTIONS FOR SUBMITTING TICKS:
Was the tick attached? Yes_____ No_____ Date Collected:________________________________ Ohio County where tick exposure Occured:_________________ Tick was on: Human:____ Animal:____ What kind?___________ Other Surface:___________________________________________ Describe:________________________________________________ Patient/Collector's Name:____________________________ Age: ______ Sex: ______ Address:_________________________________________________ City:_________________________ State:______ Zip:_________ Phone: ______________ Send Results To: (if different from patient) Name: ___________________________ Age: ______ Sex: ______ Address:_________________________________________________ City:_________________________ State:______ Zip:_________ Phone: ______________
IMPORTANT NOTE: TEST results are NOT DIAGNOSTIC. If you think you have a tick-borne disease, seek medical attention. Do not wait for test results.