Good Reads on Cord Complications HOME
**Please see bottom for pictures of Nucal Cord.**
Nuchal Cord / Cord Entanglement
With Nuchal Cord, the cord becomes coiled around
various parts of the body of the fetus, usually around the neck. Nuchal Cord is
caused by movement of the fetus through a loop of cord.
One loop around the neck occurs in approximately 20% of
cases, and multiple loops occur in fewer than 2 per 1000 cases.
This can be detected using color Doppler Ultrasound,
with a sensitivity of over 90% after 36 weeks' gestation.
Nuchal Cords rarely cause fetal demise and are not
intrinsic reasons for intervention.
The prenatal treatment of Nuchal Cord is controversial.
Fetal testing and Doppler studies of the cord may be instituted. As the fetus
descends during labor, the cord may become compressed, leading to fetal heart
rate decelerations. Infants with Nuchal Cords tend to have more decelerations in
labor and lower umbilical artery pH
Case Study 3 - Umbilical Cord Accidents - Time of
Death
Jason H. Collins, M.D.
Pregnancy Institute has operated a Web site since July 1996. Over 5500hits
have been recorded since its start up. One of the topics discussed is Umbilical
Cord Accidents. E-Mail from parents experienced with this form of stillbirth
began to share their case stories with Pregnancy Institute. These inquiries led
to a series of interviews now numbering 60 stillbirths. Most
of the pregnancies were term and around from the U.S. Some were from outside of
the U.S. Questions pertaining to the events that preceded the stillbirths
focused on fetal behavior and time of fetal movement prior to death. Mothers and
fathers seemed to readily remember these details and all recalled fetal movement
the day before demise. Surprisingly all deaths were associated with the mothers
sleep cycle. Most deaths occurred between 12 midnight and 7 am. Some anecdotal
events timed the deaths at between 3am - 7am. Two deaths were timed at 3pm - 5pm
during afternoon naps described as deep restful sleep.
Is it possible that these deaths were not random but the result of
physiological changes which occur during maternal sleep? Could cord entangled
fetuses be stressed to the degree where these changes are detrimental whereas
unstressed fetuses can adapt. Fetal and Maternal biorhythms suggest that there
are changes during maternal sleep. Also there are similar mechanisms which
explain occlusive stroke and occlusive coronary disease. All these events seem
to be prevalent during sleep and especially in the early morning.
Investigating this further, several cases have been observed as part of the
Perinatal Umbilical Cord Project. An example is provided of a case with a 38
week fetus with a prenatally diagnosed double Nuchal Cord. (figure 1) During
maternal sleep (R side) B/P readings q 30 min showed a decline from 120/70
(awake) to 98/53 at 3:40 am. At this time a contracture (3-4 min) is associated
with a late deceleration. An OCT the next morning resulted in a C/Section for an
abnormal fetal heart rate pattern.
The possibility exists that circadian rhythms may be detrimental to the stressed fetus. In particular, maternal sleep may be associated with maternal hypotension and fetal hypoxia. As with compromised vascular states which can lead to stroke and coronary occlusion during sleep, the same principles may be affecting the cord entangled fetus.
Sited from Pregnancy Institute: Case Study of Umbilical Cord Accidents & Time of Death - http://www.preginst.com/Case_Study/case_study_3.html
Ultrasound diagnosis of quintuple nuchal cord
entanglement and fetal stress
Sandra
Rejane Silva, MD, Philippe Jeanty, MD, PhD, Cheryl Turner, RDMS, Lynn Driver, MD
Women’s Health Alliance, Department of Ultrasound, 300 20th Avenue North,
Nashville, TN 37203-2131
Abstract
We
report a case of quintuple nuchal cord found by ultrasound at 36 weeks in a
fetus with decreased movement and variable decelerations. Because of the
prenatal diagnosis of intermittent cord compression, the fetus was delivered by
C-section with excellent outcome.
The
importance of nuchal cord on the management of third trimester pregnancy and
labor has been debated for many years. The presence of a single loop of nuchal
cord may be associated with variable fetal heart rate decelerations but does not
compromise fetal well-being, and thus does not alter standard management.
Multiple nuchal cord, especially four or more loops, demands special care due to
the risk of intermittent cord compression. If signs of fetal stress are
superimposed, an operative delivery may be required. We present the ultrasound
findings, management, and outcome in a case of a five-loop nuchal cord.
The
patient was a 25-year-old woman, G2P1, at 36 weeks and 3 days of gestation,
referred for biophysical profile, due to decreased fetal movement, variable
decelerations, and non-reactive non-stress test. The prenatal care and her past
history were unremarkable.
The
exam demonstrated normal amniotic fluid, decreased fetal movement, and no
breathing. On color-Doppler, five loops of cord were wrapped around the neck
(fig. 1).
Figure
1: Sagittal section demonstrating 5 loops of cord. The ends of the cord are
divergent, supporting the idea of a Type A loop.
On
pulse-wave Doppler, the systolic to diastolic ratio was normal at 2.5. As far as
we could assess, this was a Type A looping (see below). The presentation was
cephalic and the placenta’s location fundal. Since there was no other reason
for the presence of variable decelerations and decreased fetal movement, we
concluded that the baby was strangling himself as he was pulling on the cord,
causing frequent cord compression.
Indications
for induction of delivery included a poor biophysical profile score, a
non-reactive stress test, and the nuchal cord. The patient was delivered at 39
weeks and 2 days gestational age. A C-section was performed and the prenatal
diagnosis confirmed. The 2290g male baby had Apgar scores of 9/9 at 1 and 5
minutes, and did not require any special care at the nursery. The infant was
discharged home the next day.
The
assumption that nuchal cord entanglement could cause cord compression and thus
intrapartum complications is not recent. In 1896, Gould mentioned Hippocrates’
references on nuchal cord. Hippocrates described in the “De Octimestri Partu”
the nuchal and chest coiling of the umbilical cord, and regarded it as “one of
the dangers of the eighth month”. He also stated that when the nuchal cord
persists until the term of pregnancy, it will cause suffering to the mother and
either perish or born difficulties to the fetus. Other scholars from the
Classics in Medicine consider that the “De Octimestri Partu” was not from
Hippocrates but by an unknown disciple.
Gould
also cited cases of multiple nuchal cord and described stillbirths probably
related to severe cord compression1. In reviewing his text, some cases appeared
to be simply amniotic band syndromes, but others appeared to be genuine cord
strangulation.
Nuchal
cord is present in one-fourth of pregnancies but generally does not have major
clinical significance. According to Larson, the occurrence of nuchal
entanglement increases linearly from 5.8% at 20 weeks of gestation to 29% at
42weeks. The presence of two or more loops is estimated to affect between 2.5%
to 8.3% of all pregnancies.
Giacomello
classified the nuchal cord into two types:
·
Type A - nuchal loop that encircles the neck in a freely sliding pattern (fig.
2)
·
Type B - nuchal loop that encircles the neck in a locked pattern (fig. 3)
Thus,
type A can undo itself, while type B cannot.
Figure
2: Type A loop: a nuchal loop that encircles the neck in a freely sliding
manner. Should this fetus be delivered breech, the loop can slide off the neck
of the fetus.
Figure
3: Type B loop: a nuchal loop that encircles the neck in a locked manner. Should
this fetus be delivered breech, the loop will get tighter around the neck of the
fetus.
The
recognition of a single loop relies on the observation of a section of cord
between the head and shoulder in a sagittal section, and the demonstration of a
complete loop in an axial section of the neck. This is often difficult because
of shadowing, and a compound image is often required. In an axial section, cord
that is simply draped over the neck can be excluded. Color Doppler is the
easiest mean to assess the cord in the axial view. Multiple loops are detected
in the same manner, but the number of loops can only be counted in the sagittal
section. Again, color Doppler is the easiest modality to count multiple loops.
The assessment of the type (locking versus freely sliding) requires the
demonstration of the crossing of one of the ends under the other end. This is
easier in higher order looping since the cord is more taught, but if the
crossing occurs behind the fetus, the diagnosis cannot be made.
Despite
the good prognosis in most of the cases, some studies demonstrate that the
presence of a nuchal cord is associated with variable fetal heart rate
deceleration, decreased fetal movement, umbilical arterial metabolic acidemia,
neonatal anemia, and, in extreme situations, intrauterine fetal demise.
In
1995, Larson, studying intrapartum complications associated with multiple nuchal
cord entanglement, concluded that the group with four or more loops involved had
significantly lower birth weight, more episodes of severe variable and late
decelerations, meconium, and a higher incidence of operative delivery5.
Multiple
nuchal cord is probably the most common of abnormal umbilical cord
findings. Variable decelerations commonly occur during the first and second
periods of labor. When episodes of cord compression are sufficiently spaced, the
fetus can clear the increased CO2 and maintain the
oxygenation by using the oxygen reserve. However, if signs of fetal discomfort,
such as decreased fetal movement or persistent fetal heart variable
decelerations, or even signs of fetal distress like repeated late decelerations
are present, operative intervention is recommended.
We
speculate that, in the present case, the good Apgar scores and outcome at the
nursery are attributed to the prompt intervention on the ultrasound findings.
Although
the presence of a single nuchal cord does not require changes on the management
of the pregnancy, the prenatal detection of multiple loops may alter the
management and improve the outcome of these fetuses.
Our
experience and the literature show that most cases of four or more nuchal loops
are at high risk to develop complications in labor and delivery; thus, these
cases demand caution and are more likely to end in an operative intervention.
Sited
from Fetus.net: Nuchal Cord Entanglement and Fetal Stress -
http://www.thefetus.net/page.php?id=172
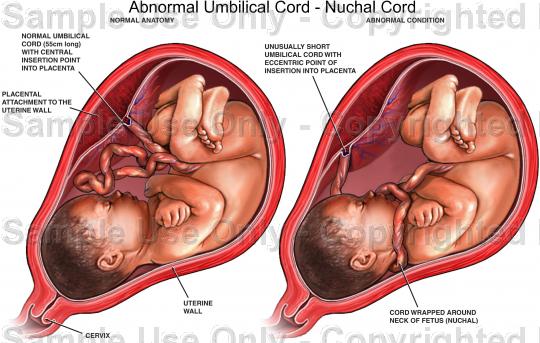
Nucal Cord (cord entangled around neck) & unusually short umbilical cord
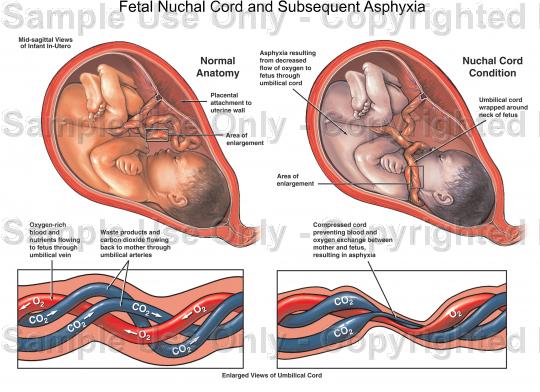
Nucal Cord and subsequent asphyxia (strangulation).
Sited from: http://www.doereport.com/generateexhibit.php?ID=347