![]()
|
|
|
I stole all of this from http://www.kcenter.org/Keratoconus/what_is_keratoconus.html thru the magic of Cut and Paste
KERATOCONUS Keratoconus has no known cure, and many people do not even know they have it because it begins as nearsightedness and astigmatism. It is a progressive disorder that may progress rapidly or sometimes take years to develop. It can severely affect the way we see the world, including simple tasks such as driving, watching TV, or just reading a book. Some keratoconus patients have described their vision as being “blind with light.” Keratoconus is a non-inflammatory, self-limiting ectasia of the axial portion of the cornea. It is characterized by progressive thinning and steepening of the central cornea. As the cornea steepens and thins, the patient experiences a decrease in vision which can be mild or severe depending on the amount of corneal tissue affected.
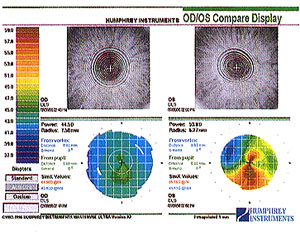
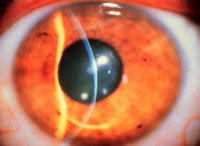
Onset of keratoconus occurs during the teenage years--mean age of onset is age 16 years--but onset has been reported to occur at ages as young as 6 years. Keratoconus rarely develops after age 30 years. Keratoconus shows no gender predilection and is bilateral in over 90% of cases. In general, the disease develops asymmetrically: diagnosis of the disease in the second eye lags about five years after diagnosis in the first. The disease process is active for about five to 10 years, then it may be stable for many years. During the active stage, change may be rapid. Typically, vision loss can be corrected early by spectacles; later, irregular astigmatism requires optical correction with rigid contact lenses. Contact lenses provide a uniform refracting surface and therefore improve vision. Contact lenses can improve vision, but they can also scar the cornea. Patients should be informed upon diagnosis that they will likely require contact lenses eventually. Although most patients can continue to read and drive, some feel quality of life is adversely affected. Patients need to know that eye examinations will be required annually or more frequently to monitor progression. About 20% of patients will eventually need a corneal transplant. Etiology The proposed etiology of keratoconus includes biochemical and physical corneal tissue changes, but no one theory fully explains the clinical findings and associated ocular and non-ocular disorders. It is possible that keratoconus is an end result or final common pathway of many different clinical conditions. It has been found in association with hereditary predisposition, atopic disease, certain systemic disorders, and long-term rigid contact lens wear. Diagnosis Identifying moderate or advanced keratoconus is fairly easy. However, diagnosing keratoconus in its early stages is more difficult, requiring a thorough case history, a search for visual and refractive clues and the use of instrumentation. Often, keratoconus patients have had several spectacle prescriptions in a short period, and none has provided satisfactory vision correction. Refractions are often variable and inconsistent. Keratoconus patients often report monocular diplopia or polyopia and complain of distortion rather than blur at both distance and near vision. Some report halos around lights and photophobia. Many objective signs are present in keratoconus. Retinoscopy shows a scissoring reflex. Direct ophthalmoscopy may show a shadow (Fig. 1). If the pupil is dilated and a +6.00 D lens is in the ophthalmoscopic system, the cone may appear as an oil or honey droplet when the red reflex is observed. Fig 1. The keratometer also aids diagnosis. The initial keratometric sign of keratoconus is absence of parallelism and inclination of the mires. These can easily be missed in mild or early cases. As the cornea advances, the mires appear smaller. To extend the range of the keratometer, an ancillary lens is placed on the front of the keratometer . If a +1.25 D lens is used, this extends the range to 60 D. To record a reading, 8 D is added to the drum reading (for example, if the drum reads 45 D, adding 8 D yields an actual reading of 53 D). A +2.25 D lens extends the range to 68 D by adding 16 D to the reading. The photokeratoscope or topographer placido disc can provide an overview of the cornea and can show the relative steepness of any corneal area. Figure 2 depicts the keratoconic cornea. The even separation of the rings in the spherical and the astigmatic cornea and the uneven spacing of the rings--especially inferiorly--in the keratoconic cornea should be noted. The central rings may show a tear-drop configuration termed "keratokyphosis". Reduced visual acuity in one eye, due to the disease's asymmetry, may be a clue with the early keratoconus patient. This sign is often associated with oblique astigmatism. In early keratoconus, the patient may become less myopic six months later as the astigmatism increases.
Keratoconus can result in extremely complex and variable topographical maps, most typically showing areas of inferior steepening. The cone can assume various shapes and sizes, and the apex can be at various locations in relation to the central cornea.
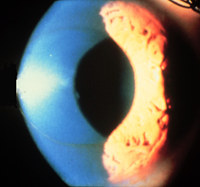
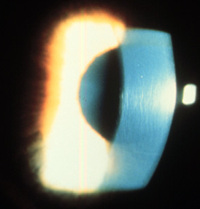
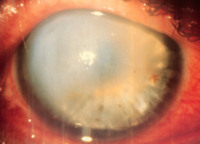
SLIT-LAMP DETECTION The biomicroscope is the only tool which allows a clinician to observe many classical signs of keratoconus: Fleischer's ring, stress lines of Vogt, corneal thinning and scarring, various types of staining with and without lens wear, increased visibility of corneal nerves, and corneal hydrops. Fleischer's Ring The Fleischer ring is a yellow-brown to olive-green ring of pigment which may or may not completely surround the base of the cone (Fig. 3). Formed when hemosiderin (iron) pigment is deposited deep in the epithelium , Fleischer's ring often becomes thinner and more discrete with progression. A careful inspection of the keratoconic cornea will reveal a line in approximately 50% of all cases. Locating this ring initially may be made easier by using a cobalt filter and carefully focusing on the superior half of the cornea's epithelium. Once located, the ring should be viewed in white light to assess its extent. Fig 3. Lines of Vogt Lines of Vogt are small and brush like lines, generally vertical but they can be oblique. These lines can be found in the deep layers of the keratoconic stroma (Fig. 4) and form along the meridian of greatest curvature; the lines disappear when gentle pressure is exerted on the globe through the lid. Lines of Vogt are more easily viewed when they reappear after this pressure is removed. Rigid lens wear sometimes accentuates the lines. In advanced cases of keratoconus, posterior corneal folds may also be present. Fig 4. Corneal Thinning Significant thinning (up to 1/5th cornea thickness) in the advanced stages of the disease (Fig. 5), and a diagnostic criterion based on comparison of central and peripheral corneal thickness has been proposed. Additionally, as the disease progresses, the cone is often displaced inferiorly. The steepest part of the cornea (apex) is generally the thinnest. Apical thinning described is believed to represent an actual reduction in the number of stromal lamellae rather than an overall thinning process. Fig 5. Corneal Scarring Sub-epithelial corneal scarring, not generally seen early, may occur as keratoconus progresses because of ruptures in Bowman's membrane which is then filled with connective tissue (Fig. 6). Deep opacity of the cornea are not uncommon in keratoconus. It has also been reported that flat-fitting contact lenses may produce or accelerate corneal scarring. A raised "callous" is possible but is easily treated by simple debridement or laser ablation. In addition, apical scarring with an overlying epithelial defect and surrounding edema can be confused for ulcerative keratitis in this disease process. Fig 6. Swirl Staining Swirl staining may occur in patients who have never worn contact lenses because basal epithelial cells drop out and the epithelium slides from the periphery as the cornea regenerates. Thus, a hurricane, vortex, or swirl stain may occur (Fig. 7). Swirl staining may be due to rubbing of the eye or can also result from flat- fitting contact lenses. When this is the case, the lens is generally too flat. A steeper lens often diminishes staining. Fig 7. Hydrops Corneal hydrops occurs, generally in advanced cases, when Descemet's membrane ruptures, aqueous flows into the cornea and reseals (Fig. 8). Keratoconus patients who are having an acute episode of corneal hydrops report a sudden loss of vision and a visible white spot on the cornea. Corneal hydrops causes edema and opacification. As Descemet's regenerates, edema and opacification diminish. Occasionally, hydrops can benefit keratoconus patients who have extremely steep corneas. If the cornea scars, a flatter cornea often results, making it easier to fit with a contact lens. An increased incidence of hydrops has also been reported in keratoconus patients with Down's syndrome. Excessive rubbing should be discouraged in this population. Anecdotally, hydrops seemed to be more prevalent when scleral lenses were employed as a treatment option. Fig 8. Munson's Sign Munson's sign is readily observable without using the slit lamp (Fig.9). This sign occurs in advanced keratoconus when the cornea protrudes enough to angulate the lower lid during inferior gaze. Fig 9. Ruzutti's Light Reflex A light reflex projected from the temporal side will be displaced beyond the nasal limbal sulcus when high astigmatism and steep curvatures are present. Although not a pathognomonic sign, Ruzutti's reflex may aid in a diagnosis especially when a biomicroscope or other tools to aid in diagnosis are not available. Reduced Intraocular Pressure A low intraocular pressure is generally found. This is a result of a thinner cornea and/ or reduced scleral rigidity. Due to possible artifact and since the reliability of readings are in question caution must be taken in carefully observing nerve fiber layers and the overall health of the optic nerve. Classification Keratoconus can be classified by cone shape, central keratometric reading, or progression. The simplest classification systems are based on keratometric reading or shape: Based on severity of curvature
Based on shape of cone
Surgical Treatments Various types of surgery are available for the patient with keratoconus. Penetrating keratoplasty is the most common. In this procedure, the keratoconic cornea is prepared by removing the central area of the cornea, and a full-thickness corneal button is sutured in its place Usually, trephines between 8.0-8.5 mm are used. Fleischer's ring can be used as the limit of the conical cornea. Generally, the second eye is not grafted until the first eye is successfully rehabilitated. Running sutures, using Merseline, anchored by cardinal sutures provide excellent results (clear, compact grafts). Older patients with a slower healing response and altered tear film generally do better with nylon and interrupted sutures for selective removal. Contact lenses are often required after this procedure for best visual correction. An alternative is lamellar keratoplasty, a partial corneal transplant. The cornea is removed to the depth of posterior stroma, and the donor button is sutured in place. This technique is technically difficult, and visual acuity is inferior to that obtained after penetrating keratoplasty. As a result, use of lamellar keratoplasty is largely confined to the treatment of large cones or keratoglobus when tectonic support is needed. This technique requires less recovery time, and poses less chance for corneal graft rejection or failure. Its disadvantages include vascularization and haziness of the graft. Excimer laser procedures may have some potential merit, having been used recently with some success in removal of nodular "callous" plaques of the central cornea. New developments in excimer corneal modeling may allow lamellar onlay or penetrating grafts to be lathed, thereby eliminating refractive ametropia following various surgical procedures. |
|
If you want to contact me I can be reached by email and chat
|