NASH'S
"DILLINGER: DEAD OR ALIVE"
TRUTH OR FICTION?
By Bob Fischer
Since Dillinger’s demise at the hands of the G-men there have been those who believe that he somehow escaped his fate yet again. It began with reports of how different the man killed looked. Even when his sister, Audrey Hancock, identified the body as John, the rumors continued. In modern times this story continues to have its proponents. Most of these individuals arrived at their belief after reading Jay Robert Nash’s 1970 book, DILLINGER: DEAD OR ALIVE. No less an author than Anthony Summers gives Nash unquestioning credence in his 1993 book OFFICIAL AND CONFIDENTIAL: THE SECRET LIFE OF J. EDGAR HOOVER.
Don’t get me wrong, I love a good conspiracy theory as much as the next guy and as these types of books go, Nash’s is one of the best. I won’t attempt a full fledged review here, let it suffice to say that the first part of the book is both as riveting as a good detective story and as entertaining a book of this type could hope to be. The second half, on the other hand, falls apart under the weight of its hyperbolic notions and overwrought prose, but that is beside the point. It's basically fun reading, the problem is, the book isn't true. I won't attempt a line by line critique of Nash's evidence. My approach instead will be to tackle one area in particular, i.e., the evidence presented in the autopsy report that points to Dillinger having had heart disease in consideration of Nash's unequivocal denial that Dillinger did not have heart disease. If Nash's observation were true it would give considerable weight to his theory that the FBI killed the wrong man.
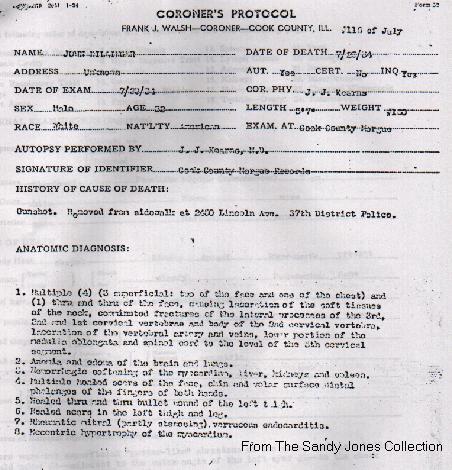
Let me begin by stating that I am not a doctor and have no medical background so that makes me at least as qualified as Mr. Nash to analyze the autopsy information presented in Dr. J.J. Kearns' 1934 autopsy of Dillinger. Kearns described the dead man's heart this way:
Anatomic diagnosis 7. "Rheumatic mitral (partly stenosing) verrucose endocarditis"
Anatomic diagnosis 8. "Eccentric hypertrophy of the myocardium"
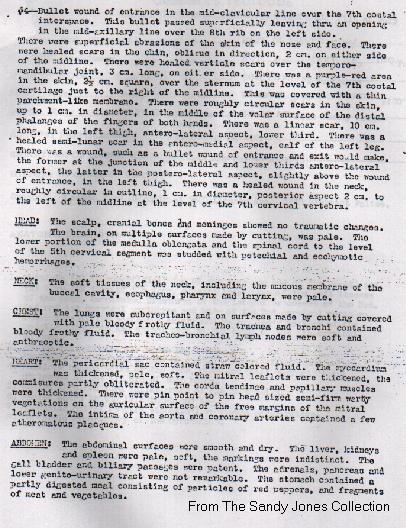
Heart: "The periocardial sac contained straw colored fluid. The myocardium was thickened, pale, and soft. The mitral leaflets were thickened, the commisures partly obliterated. The corda tendinae and papillary muscles were thickened. There were pin point to pin head sized semi-firm warty vegetations of the auricular surface of the free margins of the mitral leaflets. The intima of the aorta and coronary arteries contained a few atheromatous placques."
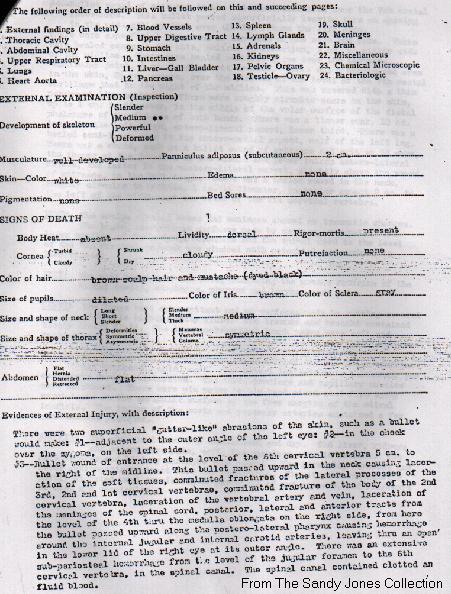
Autopsy report on John Dillinger
page 1
page 2
page 3
{kind=link}
{kind=link}
{kind=link}
Nash correctly identifies the "Rheumatic" Mitral Stenosis as being the result of a bout of Rheumatic Fever. He then states unequivocally that Dillinger never had Rheumatic Fever and that if he had "it is highly unlikely he would have been able to play a strenuous game of baseball, as Dillinger certainly did both in Martinsville and in prison." Nash then states that "it is almost impossible to believe that he [Dillinger] would be accepted into the U.S. Navy with such a condition".
A look at the standard physician's medical reference, The Merck Manual of Diagnosis and Therapy 15th and 18th editions, provides information on Rheumatic Fever and its complications. First of all there are five major manifestations which "can appear alone or in combinations". One of these is Carditis, which is defined as "inflammation of the heart including pericarditis, myocarditis, and endocarditis, according to whether the enveloping outer membrane, the muscle, or the inner lining is affected." More on endocarditis shortly. In Rheumatic Fever "a patient with carditis will seek medical attention only if sufficiently febrile [feverish], if pericarditis is present and painful, or if hear failure produces respiratory, peripheral, or abdominal manifestations. In the absence of these provocations, the cardiac damage may not be discovered until much later, when the patient is found to have 'rheumatic heart disease without a history of rheumatic fever'"(15th edition). [Italics mine]. Significantly as it applies to Dillinger, " in about 50% of affected adults, the cardiac damage may not be discovered until much later". [Italics mine] In essence these two statements demonstrate how Dillinger could have had undetected heart problems from a case of Rheumatic Fever undermining Nash's categorical claim that he could not have had the disease.
The reference Kearns makes to Mitral Stenosis, which is defined as "obstruction of flow from the left atrium to left ventricle because of narrowing of the mitral orifice" involves a description of a specific heart problem caused by Rheumatic Fever. Again according to The Merck Manual, "In temperate climates the latent symptom-free period may last 10 to 20 years; symptoms usually begin between ages 30 and 40. Significant mitral stenosis is often found in patients with minimal or no symptoms". John Dillinger was 31-years old at the time of his death.
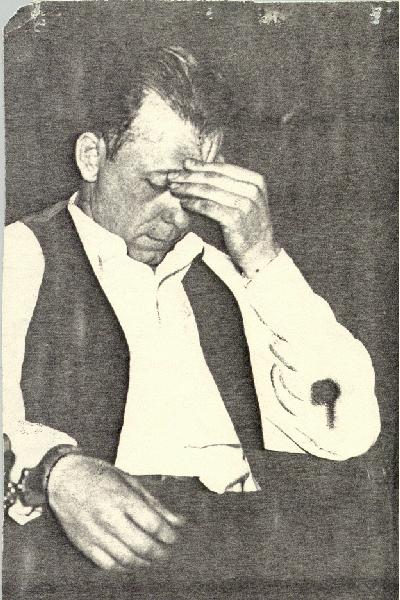
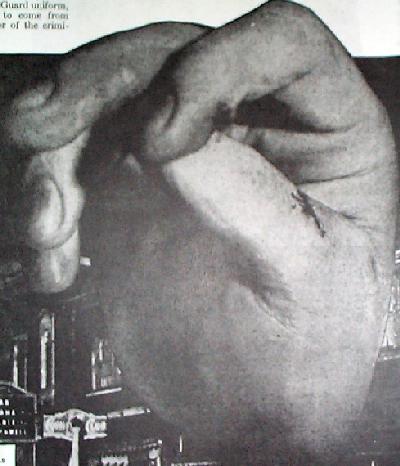
Kearns mentions Verrucose [warty] Endocarditis in his description of the mitral valve in association with the stenosis. It would appear that Kearns is referring to the non-infective type in his report. It is also related to Rheumatic Fever. The Merck Manual states that noninfective endocardial vegetations "tend to form more often on abnormal cardiac valves damaged by rheumatic fever...they are most common on the mitral valve". Although not specifically associated with the non-infective form of endocarditis, it would appear that, possibly as a result of Dillinger's enlarged heart (the hypertrophy of the myocardium mentioned by Kearns) and rheumatic fever related heart damage, Dillinger may have been exhibiting the early stages of a condition known as "clubbing of the fingers". This can be determined from studying photographs of Dillinger's hands. Of significance to disputing Nash's claim that the corpse was not Dillinger is the fact that a close-up of the hand of the corpse, identified by the authorities as Dillinger, exhibits this same condition.
The technical description of this condition would seem to describe the look of John's fingers perfectly. Dillinger’s hands, which were photographed in close-up while under arrest and after death, display this characteristic of long and sunken fingernails very clearly. Nash makes no mention of this whatsoever. *See medical description of "Clubbing" below.
Clubbing by Paul B Cornia, MD and Gregory J Raugi, MD, PhD
Clubbing, a term used to describe the bulbous, club-like deformities of the digits resulting from proliferation of the connective tissue of distal parts of the fingers and toes, may have been first described by Hippocrates. Patients with this finding are sometimes said to have "Hippocratic fingers." Clubbing can be hereditary, idiopathic, or associated with a number of different conditions including congenital heart disease, infective endocarditis, and many pulmonary diseases such as pulmonary arteriovenous malformations, lung cancer, lung abscess, bronchiectasis, cystic fibrosis, and several interstitial lung diseases. Clubbing is an unusual finding in chronic obstructive pulmonary disease and should prompt a search for other causes.
Although the pathogenesis of clubbing is poorly understood, the end result seems to involve increased blood flow to the distal phalanges. Histopathologic studies have shown no difference in the number or length of vessels, indicating that the increased blood flow is likely due to local vasodilation.
Clubbing results from proliferation of the connective tissue of the distal portion of the digits.
Finally, the connective tissue proliferation results in a "spongy" quality to the proximal nail fold, as if the nail were floating in the nail bed. This is used to distinguish secondary clubbing from hereditary clubbing which lacks this quality.
And from the Merck Manual:
Clubbing of the fingers
Enlargement of the terminal digital phalanges with loss of the nail bed angle.
Clubbing of the fingers is seen in a variety of conditions, including cyanotic congenital heart disease and a number of pulmonary diseases. Occasionally, it is congenital and unassociated with any disease. Among pulmonary diseases, lung tumors and chronic septic conditions (e.g., bronchiectasis or lung abscess) are most commonly associated with finger clubbing. Shunting in the lung (e.g., that associated with an arteriovenous fistula) may cause clubbing. Tumors associated with finger clubbing are usually malignant, but clubbing has been reported in patients with benign fibroma of the lung or pleura. Finger clubbing is not commonly seen in patients with chronic obstructive pulmonary disease or chronic pulmonary TB; if it appears in such patients, a tumor may be suspected.
(As stated at the beginning of this piece I am not a doctor nor do I play one online so if there is a cardiologist in the house I would like to hear from you.)
On an additional point, Nash makes an issue of the weight difference between the March 12, 1934 FBI Identification Order which lists Dillinger's weight as 156 lbs. and the weight listed by Coroner Kearns on the autopsy report of 160 lbs. Nash points out that Dillinger's naval records from 1923 list 153 lbs., a difference of 3 lbs. from that date until the March 1934 date. He then suggests the unlikelihood of a 7-pound increase from March 12 until his death on July 22. A seven-pound weight gain in four months is not out of the question for a 31-year old man but does seem unlikely. The problem with Nash's assessment lies in putting too much faith in the information contained in the FBI document. There is no indication of how or when the FBI obtained the data contained in the IO. I should note that it is curious that Nash, who doubts the FBI so vigorously elsewhere, doesn't question this information. A photographic comparison of Dillinger between the time of his initial incarceration at Michigan City in 1929 and his arrest photo from Tucson suggests more than a three-pound difference. Lastly, a quick look at the data on the back of Dillinger's 7/22/33 Muncie, Indiana, mugshot indicates his weight at the time of Dayton, Ohio, arrest as 160 1/2 lbs., which if true, raises serious doubt about Nash's argument on this issue.
{kind=link}
One final note that I can't resist regards Nash's claim that Dillinger was missing his "right top incisor" [right top lateral incisor] but the dead man identified as Dillinger in the Cook County Morgue was not. Further proof, Nash cites, that it was not Dillinger. This assertion requires the dark photographic print quality of the illustrations in Nash’s book to be believed at all. Additionally, it appears that Nash has incorrectly identified the tooth in question. The position of what appears to be a bad tooth or a gap in photos of Dillinger smiling would suggest the right upper canine. The photo in Nash's book of the dead man does not even show the mouth open far enough to show the canine area. I have included here, a blowup of John's face from the famous Mooresville "wooden pistol" shot, properly oriented and showing Dillinger’s right top lateral incisor and what appears to be a gap (between the lateral incisor and canine)or bad right upper canine tooth in all of their glory.

Suffice it to say that all of Nash's evidence can be similarly overturned on close scrutiny. For all of Nash's magnificent nonsense, however, he did come up with some interesting information. He proved that the gun held by the FBI (a .38 caliber Colt automatic) was first sold 5-months after Dillinger's death! He did turn up Kearn's long lost report and Anna Sage did know Martin Zarkovich long before the Biograph incident. According to FBI documents the FBI found out about this link after the setup. In fact the real conspiracy story in the Dillinger case is how the East Chicago Mob set up Dillinger through a crooked cop and mutual acquaintance to die at the hands of the G-men. It would even appear that this very same cop, completely out of his jurisdiction was allowed to participate in and probably insure the death of Dillinger at the Biograph trap. For more on this I would recommend Girardin and Helmer's DILLINGER: THE UNTOLD STORY. Oh, and just one more thing, Mr. Nash, if you are out there, could you sign my copy of your book?
© 2001 Outlaw Archives
|
|
Leave Message or Comments
View Messages and Comments
![]()
Get your own Free Home Page