FROM HEALTHY BUILDINGS TO HEALING BUILDINGS
Dr Ruzica Bozovic-Stamenovic1, Dr Ong Boon Lay2 & Ismail Said3
ABSTRACT1 Assistant professor, Department of Architecture, National University of Singapore
2 Senior lecturer, Department of Architecture, National University of Singapore
3Associate professor, Department of Landscape Architecture, University Technology of MalaysiaThis paper will be presented at Healthy Buildings 2003 Conference July 13-17, 2003 at National University of Singapore.
A new paradigm for healthcare design is needed. Usually designed for efficiency and cleanliness, healthcare spaces need to accommodate the notion of eustress (or positive stress) as a significant contributor to healing. The engagement of senses is essential in facilitating the transition from healthy buildings to healing environments. This paper reviews current research and presents original findings by the authors. Sensory stimulation design is proposed as an amalgam of innovative design solutions related to spatial cognition. Guidelines are discussed and illustrated by some original solutions. Special consideration is given to healing landscapes. These landscapes arouse positive feelings towards the healthcare settings and foster the restorative or healing process. A case study of therapeutic gardens in recuperation of acutely ill children in two nucleus hospitals in Malaysia is presented.
Keywords: healthy buildings, healing, eustress, landscape, architecture, sensory stimulation design
INTRODUCTION
The transition from healthy buildings to healing buildings is based on the recognition of the dual character of health. According to WHO: Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. Being part of the complex entity of nature, man possesses an immanent, balanced, subconscious relation to the environment that is nurturing both its physical and astral body.
The present paper proposes a paradigm shift in healthcare building design from a concern with health to a concern with healing. Recent research has emphasized the importance of the psychological state of mind of the patient and a supportive environment in the process of healing. In order to place the two concerns in a complementary framework, we propose on the one hand, a concern for health which may be regarded as the state of being healthy and free from illness; and on the other hand, a concern for healing, which is the process of moving from illness to a state of health.
STRESS - DISTRESS AND EUSTRESS
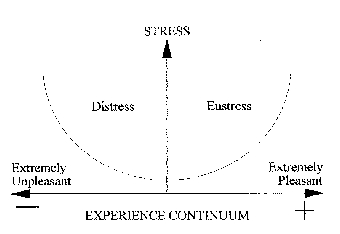
Although stress is widely discussed in our society, we understand stress only in its negative sense. Hans Selye (1956/76, 1974), the originator of the concept of stress, saw stress as a natural and essential component of living. He identified two kinds of stress distress and eustress (Fig. 1). For most of us, all stress is distress. But stress can also be positive. Many of us are familiar with the experience of being able to withstand high levels of stress (little sleep, extensive traveling, exposure to the elements) during our vacations with little negative effects. On the other hand, we could be stressed out, or rather, to use Selyes terminology, distressed without much external physical stress from the environment (we can be either in the office or at home most of the time) and yet falling sick easily.
Figure 1: Stress as an experience continuum. Any deviation from the norm is stressful but there can be positive stress as well as negative stress (adapted from Selye 1974).
The significance of this psychological aspect of stress is widely recognized both in research on stress as well as a form of coping with stress. One common method of dealing with stress is to find some relief from stress through quiet and spending time with supportive friends and relatives. But we can also escape stress by doing something physically demanding like swimming or exercise that we enjoy. Indeed, for many people, this physical activity, because of its ability to focus our minds on the activity and thus remove the worry, is more effective than finding a quiet environment. In a quiet environment, we may worry even more!Another common strategy in coping with stress is to try to look at the distressful event objectively. In a sense, the aim is to look at some of the positive aspects of the worry. What is happening here is an attempt to convert distress to eustress, from negative stress to positive stress.
1 Environments for eustress
The architecture translation of this idea is to design sensory stimulating environments. By designing environments that are stimulating in a positive way, patients are cheered up and psychologically encouraged to get better. There are two aspects or main approaches to designing sensory stimulating environments. The first is architectural looking at building design and the design of components: (railings, doors, façade components, etc). The second is landscape using plants as positive motivators to healing through active involvement with the landscape and sensory stimulation.The following sections present original research work in both these areas.
SENSORY STIMULATION DESIGN
Physical characteristics of space like dimensions, ergonomics, quality and safety of the materials used as well as functional features allow for the appropriate and safe utilization of spaces. However, healthy spaces designed in this way have not necessarily been found to have a healthy influence on mental capacities of the users. Illustrative example is the common use of glossy materials for floors in healthcare spaces. Although clean and easy to maintain they are a hindrance to the patients motor capabilities. Most common initial response to the environment is not at the intellectual level, but rather an emotional one. Successfully creating a healing building means addressing this duality.
Architectural design is a dynamic, intentional process of structuring matter and energy in space and time. Physical reality and metaphysical manifestations of space are detected through the senses and reflected as emotions about the space. We discuss sight, sound, touch, smell and taste as sensations but their major effect manifested in space is their irrevocable interdependence. Even the common English expression I see implies much more than just visual information. Abilities connected to spatial cognition are dependent on multiple factors like gender, age, cultural and educational background, social patterns or personality in general (as argued by Carl Jung). Sensory stimulation design has to scientifically sanction issues of: resultant sensory effect, dominant components, legibility and influence, flexibility and control, etc.
1 Guidelines for sensory stimulation design
The lack of legislation and guidelines in this area of design is self-evident. Further research is needed to articulate recommendations and/or set of formulas to express the required level of sensory stimulation. These guidelines should reflect:- Scientifically measured and controlled outcomes through a multidisciplinary approach. Relevant research from disciplines like psycho-neuro-immunology (PNI), phenomenology, and environmental psychology provide viable tools. Evaluation of sensory stimulation design should also consider relative components like number of stimuli, intensity, relative quality, appropriateness, level of control, etc.
- Potentials and applicability The guidelines should also provide for the new solutions to be able to adjust to changing demands. Initial investment in typical hospital represents only two percent of the total expenditure over a typical 30 years life cycle. This consideration has an impact on other disciplines too, like building technology and industry.
1.1. Examples of sensory stimulation design:
1. Louvers are extensively used in the Tropics as an environmental tool. Their form is
without exception linear, longitudinal, sometimes with regular perforations. However, research on nature and healthcare environments found that organic forms are perceptually related to natural forms and are better received by many patients. Such forms can compensate for the literal lack of greenery. By altering the form of louvers to an organic and irregular design, patient acceptability is improved by:
a) dissolving the otherwise sharp edge between the built and the natural;
b) making the view more interesting, surprising and inspiring;
c) allowing for organic shape and color of reflected shadows, etc.2. Handrails are usually designed as a linear element of constant height and so are not
adapted to the different heights of users.
Figure 2: Original design by Bozovic-Stamenovic of S Line handrail based on ergonomic analysis of human walk
A S LINE handrail (Fig. 2) is not only more practical in catering to the different comfortable hand holding positions of the users but is at the same time a therapeutic tool and sensory stimulation device. The hand is exercised in holding the rail in different positions and at different heights.
HEALING LANDSCAPES
Although the advancement of modern hospitals has subdued the nurturing properties of nature for healing, some hospitals still value such properties and integrate their buildings with gardens and courtyards (Marcus, 1999). The integration is based on the premise that experiencing the landscape, either in a passive or active mode, reduces stress in the patients during recuperation in the hospitals.
Hospitalization often erodes the patients feelings of control due to loss of privacy, loss of control over eating and sleeping times, lack of information, and wayfinding difficulties in complex and unfamiliar hospital buildings. Young patients, especially, see the hospital as an alien setting that inflicts pain and separation from their families. Hospitalization has been found to cause regressive behavior among toddlers and young children. Some of these behavior patterns include excessive nighttime fears, increased clinging to and dependence on parents, loss of bowel and bladder control, or intensified thumb-sucking (Lindheim et al., 1972). Such stress can be ameliorated through the use of natural settings such as gardens. In their Attention Restoration Theory, the Kaplans (Kaplan, 2001) argued that the viewing of wilderness/nature can offer a restorative effect and emotional relief from the overloaded informative environment common in modern society and architectural settings that cause fatigue. Ulrich (1999) supported this theory and introduced the Stress Coping and Restoration Theory that views nature as a positive distraction that improves the emotional state of the perceiver. The positive distraction fosters beneficial changes in the physiological system such as lower blood pressure and lower stress hormones production. More positive outcomes are attained when the patients actively participate in and interact with natural features of the garden.
In terms of the healing process, therapy gardens for children can be categorized into four types: play, horticulture, nature and animal (Moore, 1999). From the perspective of physical form and quality of physiological and psychological well-being of the children, there is no discrete division between these gardens because vegetation is the common denominator in defining the spaces in the gardens. The most common type is the play therapy garden where children can practice sensorimotor play, pretend play and games with rules. This is the garden type in our case study of the gardens at Batu Pahat Hospital and Segamat Hospital in Malaysia. Both gardens are located beside the pediatric ward and can be easily accessed both visually and physically.
1. Case Study: Children Therapeutic Gardens
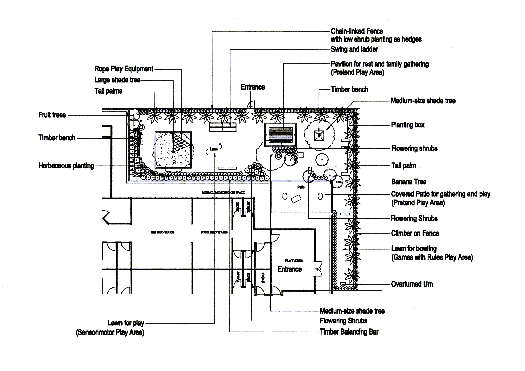
The therapeutic gardens at Batu Pahat Hospital (308 m2 Fig. 3) and Segamat Hospital (740 m2) are surrounded on three sides by two-storey buildings and overlook the surrounding landscapes. Hence, a large area of both gardens is shadowed by the buildings except in mid-afternoon. Prevailing winds often blow through the gardens providing tolerable and favorable temperatures even on a sunny day.
Figure 3: Plan of healing garden for childrens ward at Batu Pahat (design by Ismail Said)
There are four spatial zones for play and rest in BPHs garden and seven zones in SHs garden. The zones include multipurpose lawn area, play structure area, sand play area, gardening area, and resting area with timber pavilion. Since the gardens are located beside the ward and stretched half to full length of the ward, patients can easily view the gardens through glass-louvered windows. They are allowed to go to the gardens about 4.5 hours during the day accompanied by their parents or ward staff. Both hospitals administer acutely ill patients whose average length of stay is 3.1 days.The success of the garden is influenced by three aspects, (1) proper site planning of the garden that ensures hierarchy of spaces, and a sense of security and safety, (2) diversified composition of natural and man-made elements that provides a variety of play activities, either familiar or innovative, and (3) interaction with microclimatic factors like light, temperature, rain and wind.
Spatially, the gardens can both be viewed and be reached easily from the ward. Bedridden patients have a good view of the gardens through the windows. The gardens thus provide a distractions and a respite from their illnesses, thus encouraging the restorative process (Kaplan, 2001). The gardens are flooded with sunlight that allows the patients to sense the spaciousness of the outdoor with a diversity of features to stimulate and fascinate the children. The children have a selection of four to seven play zones with a variety of planting compositions and play equipment. The ability to freely choose improves the patients sense of control over the environment.
CONCLUSION
As our knowledge and understanding expands from health to healing, the role of the environment as sensory stimulation increases in importance. The research presented here demonstrates the positive effects of sensory stimulation in the healing process. In this research, design plays a dominant and contributory role. More research is needed, but the work presented here is exciting not only in its explicit relationship between the design of the environment and medical research but also in its wide applicability and conception of the built environment as a whole encompassing both architecture and landscape.
REFERENCES
Devlin, Ann Sloan. (2001). Mind and Maze-spatial cognition and environmental behaviour. Westport, London:Praeger Publishers.
Herzog, T.R., Chen, H.C., Primeau, J.S. (2002). Perception of the Restorative Potential of Natural and Other Settings, Journal of Environmental Psychology, 22, 295-306.
Kaplan, Rachel (2001). The Nature of the View from Home: Psychological Benefits, Environment and Behavior, Sage Publications, Vol.33, No. 4, July, 507-542.
Lindheim, R., Glaser H. H., and Coffin, C. (1972). Changing Hospital Environments for Children, Harvard University Press, Massachusetts.
Marcus, Cooper C. and Marni Barnes (1999). Healing Gardens: Therapeutic Benefits and Design Recommendations, John Wiley and Sons, Ins. New York.
Moore, Robin C. (1999). Healing Gardens for Children. In Marcus, Cooper C. and Marni Barnes, Healing Gardens: Therapeutic Benefits and Design Recommendations, John Wiley and Sons, Ins. New York.
Selye, Hans (1956/76) The Stress of Life McGraw-Hill, New York, London.
Selye, Hans (1974) Stress without Distress Hodder and Stoughton, London.
Ulrich, R.S. (1999). Effects of Gardens on the Health Outcomes: Theory and Research. In: Cooper-Marcus, C., Barnes, M. (Eds.). Healing Gardens: Therapeutic Benefits and Design Recommendation, John Wiley & Sons, New York, pp 27-86.
Verderber, Stephen (2000). Healthcare architecture in an era of radical transformation. New Haven, CT: Yale University Press.