|
|
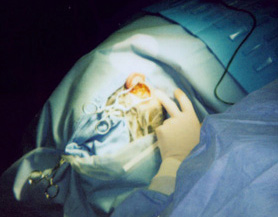
Shunt Surgery
|
|
"A postauricular incision was created 1cm posterior to the auricle and carried down through soft tissue. The periosteum was elevated anteriorly inpalva flap. Weitlaner retractors x 2 were brought in for auricular retraction. A standard cortical mastoidectomy was now initiated under constant binocular microscopic guidance with suction/irrigation and high-powered drill. Landmarks for mastiodectomy were tegmen superiorly, sigmoid sinus posteriorly, digastric ridge inferiorly, and bony ear canal anteriorly. As dissection proceeded more medially, the horizontal posterior semicircular canals were identified and skeletonized. The vertical portion of the facial nerve was likewise skeletonized with a 3mm diamond bur with constant irrigation.
The sigmoid sinus was noted to be markedly anteriorly displaced, and the approach to the endolymphatic sac was quite limited. For this reason, this sigmoid sinus was decompressed using 4mm and 3mm diamond burs and constant irrigation. An Apfelbaum retractor was utilized to hold the the sigmoid sinus posteriorly. Following this, the endolymphatic could be well visualized inferior to the posterior semicircular canal and anterior to the sigmoid sinus.
The bone overlying the endolymphatic sac was thinned with 3mm and 2mm diamond burs, the last portion was removed with a mall round knife. The wound, at this point, including middle ear space was now copiously irrigated to remove all bone dust. Under high magnification, the endolymphatic sac was incised, and the two leaves were spread with a Gimmick elevator. Silastic sheeting measuring 0.005 in thickness was fashioned into a T-shaped shunt and placed between the two leaves of the endolymphatic sac.
After ascertaining the shunt was in good anatomic alignment, retractors were removed. The sigmoid sinus was allowed to reexpand."
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |