|
A Case Report |
|
Stylianos Kornaros MD, PhD. |
|
Third Surgical Department, Tzanio Teaching Hospital, Piraeus, Greece. |
|
Valproic Acid and Pancreatitis: Which is the Mechanism? |
|
Key words: Valproic acid, Acute pancreatitis, Case report, Potential mechanism |
|
ABSTRACT |
|
Context: Pancreatitis is a rare, life threatening side effect of the use of valproic acid. However, more observations are needed to determine the frequency of this complication, as well as to elucidate any association with the potential patient subgroups. Potential mechanisms for the onset of pancreatitis have not yet been localized. Case report: A 72-year old patient was reported who, after having been treated for epilepsy for a period of two years with Valproate Sodium (500 mg/day) and carbamazepine (100 mg/day) has manifested acute pancreatitis. In this patient, no other cause of pancreatitis was found and operative intervention revealed dotted spots of necrosis in peripancreatic tissue, without any lithiasis of the gallbladder or dilatation of the common bile duct. Conclusion: Acute pancreatitis is a rare complication of valproic acid use. Efforts were made so as to explain the potential mechanism of this side effect. |
|
INTRODUCTION
Valproic acid is mainly used for the treatment of absence seizures, even though it has been shown to be effective in a wide variety of partial and generalized seizures. It is also used for the treatment of acute manic episodes in bipolar disorder and for the prophylaxis of migraine headaches. Pancreatitis associated with valproic acid has been observed in children (1,2), as well as in adults (3). Outcomes for patients with valproic acid associated pancreatitis have ranged from full recovery after discontinuation of the drug to severe hemorrhagic pancreatitis and death. The true incidence of pancreatitis associated with the use of valproic acid is still unknown. We present a case of pancreatitis, identified during an operation of the patient treated with valproate sodium and carbamazepine over a two year long period. |
|
CASE REPORT
A 72-year old man was admitted to the hospital complaining of severe abdominal pain with signs of extravagant epigastric tenderness and abdominal distension. He had been suffering from epilepsy for three years and during the last two years had undertaken a treatment which consisted of 500 mg valproate sodium (Depakine®) and 100 mg carbamazepine (Tegretol®) per day. He also received isosorbide mononitrate (Monosordil®) for his coronary insufficienciency. Laboratory tests showed an elevated serum amylase (800 IU) but also an elevation of WBC (11000), ASAT (157 IU), and ALAT (120 IU). However, bilirubin, alkaline phosphatase and γGT were normal. US and CAT examinations upon admission lacked any special evidence of abnormality in the upper abdomen. After two days, the initial diagnosis of acute pancreatitis , due to recurring and intense symptoms, was believed to be uncertain and, as a result , it was mandatory to operate on the patient. Operative findings: An abundance of fluid exudate was observed in the peritoneal cavity and especially beneath the liver. There was an edema of the pancreas, of the hepatoduodenal ligament and of the peritoneal sheet of the gallbladder. Many dotted spots of peripancreatic necrosis were noted as well as peripancreatic and epiploic fat necrosis. The common bile duct was not dilated. A cholecystectomy was performed and no signs of any lithiasis or microlithiasis of the gallbladder were found. The post-operative course of the patient, except of the left pleural effusion, were satisfactory and the patient was discharged the eleventh post-op day, with a slight elevation of γGT (158 IU), only..
|
|
DISCUSSION
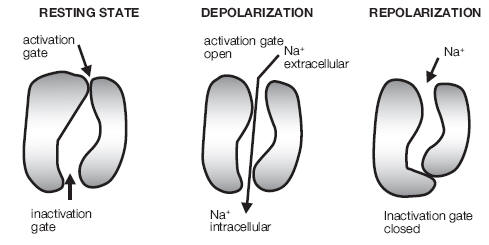
The mechanism by which valproic acid induces pancreatitis is still unknown. Depletion of the free radical scavangers, superoxide dismutase, catalase and glutatione peroxidase is estimated to be the cause of pancreatitis in a patient receiveing valproic acid (4). Valproic acid is eliminated mainly through β-oxidation into mitochondria. It has been proposed that valproic acid in pancreatitis, even it inhibits β-oxidation enzymes involved in branched-chain amino acids or an increase of toxic metabolites of valproic acid, occur, due to genetic deficiency of β-oxidation enzymes (5). On the contrary, as no change in amino acid levels in serum and urin has been observed among patients with valproic acid pancreatitis, this theory is discarded (6). The pharmacological effects of valproic acid in CNS involve a variety of mechanisms (7), including: increased gamma-aminobutyric acid (GABA)-ergic transmission, reduced release and/or effects of excitating amino-acids, modulation of dopaminergic and serotoninergic transmission, as well as prolongation of the inactivation gate closure of voltage-gated sodium channels during repolarization of nerve fiber (fig. 1). In relation to previous effects, we propose a mechanism whereby valproic acid acts on transport, mediated by carrier proteins in acinar epithelial cells of the terminal ducts of the pancreas. This action provokes changes of the protein molecules that open or close the “gates” and conformational changes of carrier proteins of Na+-K+ pump. As a result, a malfunction of primary transport or co-transport with sodium system occurs, provoking the shedding of pancreatic enzyme into intercellular space, caused by the destruction of |
|
Fig. 1: Transmitter – gated ion channels are cation channels or Cl‾ channels. The first opens by Acetilcholine, glutamate and serotonine causing an iflux of Na+ that depolarize the postsynaptic membrane. GABA or glycine open Cl‾ channels and this keeps the post-synaptic membrane polarized. Valproic acid acts through the prolongation of inactivation gate closure of the Na+ channel or through an activation of the Cl‾ channels. |