F. Rosa-Jiménez,
ÁM Montijano-Cabrera,
JJ Puente-Gutiérrez,
AM Higuera-Higuera*
Internal medicine and Radiology* Departments,
Empresa Pública Hospital “Alto Guadalquivir”,
SPAIN
Key words:
chronic hepatitis C, interferon alpha-2b,
plasminogen activator inhibitor-1,.
tissue plasminogen activator.
Abbreviations used in article:
IFN, interferon alpha; PAI-1, plasminogen activator
inhibitor-1; TGF beta, transforming growth factor-
beta; t-PA, tissue plasminogen activator
A case report
ARCH GASTROENTEROHEPATOL 2007; 26 (No 1-2)17-19
A duodenal compression
caused by the superior
mesenteric vein
ABSTRACT
We report a 64-year-old patient who was suffering from abdominal pain,
vomits, and a weight loss of two months of evolution. She showed unhealthy
general condition. The physical examination, the complete blood cell count, the
standard plasmatic biochemical analysis, a thorax and abdominal radiography,
a gastroscopy, an abdominal ultrasound, and the opaque enema were normal.
An upper gastrointestinal tract study showed a non-progression of the contrast-
medium beyond the duodenum without evidence of obstruction. An abdominal
CT indicated a compression of the third portion of the duodenum caused by the
superior mesenteric vein. The patient progress was positive with conservative
treatment.
CASE REPORT:
A 64-year-old woman, operated on nodular goiter 35 years
before, visited our hospital. She referred abdominal pain of
two months of evolution. It was located at the epigastrium
and irradiated to the right hypochondrium. It was daily and
accompanied nauseas and vomiting that got worse with the
ingestion of solid food. She had lost 5 kilos and she only ate
liquid and triturated food in small quantity due to the discomfort
that other type of feeding produced her. The patient related
that she did not have symptoms in fasting conditions with a
partial improvement after consuming antacids, spasmolytics
and omeprazol which she required everyday. The physical
examination showed an ill woman with good hydration and
no fever. Neither adenopathy nor goiter were appreciated. The
cardiac and respiratory auscultation was normal. The abdomen
was mild and depressible below the thorax and slightly painful
to the pressure in epigastrium. Hepato-splenomegaly and
abdominal mass were not found. Abdominal sounds were
abundant. She did not have edemas and peripherical pulses
were present and symmetrical. The analytical parameters
were normal (complete blood cell count, coagulation study,
hepatic and renal function, erythrocyte sedimentation rate,
thyroxin and tumour markers). The thorax and abdominal
radiography only showed slight signs of espondyloartropathy.
A gastroscopy (up to the second duodenal portion), an
abdominal ultrasound and a barium enema were informed as
normal. An upper gastrointestinal tract contrast-medium study
showed a slight duodenal dilation with a slowing-down of the
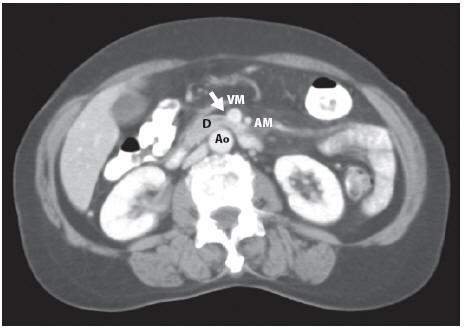
contrast medium fl ow. An abdominal computed tomography
showed a reduction of the lumen at the third duodenal portion
level in relation to a reduction in the distance between the
aorta and the superior mesenteric vein (fi gure 1). The superior
mesenteric vein presented a normal size and thrombosis
signs were not appreciated. With the diagnosis of duodenal
compression caused by the superior mesenteric vein (superior
mesenteric vein syndrome), the patient was treated with enteral
nutrition (per os). It was recommended that she distributed the
food in small and several portions and to turn into modifi ed
knee-chest position or lying on the left side after the meal. The
patient began to gain weight with this conservative treatment.
However, as a small discomfort persisted, she needed
spasmolytic medication occasionally.
DISCUSSION
The duodenal compression caused by the mesenteric
vessels has been reported in the medical literature in several
occasions (1-2). The reduction of the distance between the
abdominal aorta artery and those vessels produce that the third
duodenal portion result compressed between both of them.
This provokes an acute, chronic or intermittent obstruction
of the duodenum characterized by abdominal pain, vomiting
and postpandrial discomfort. The most frequent thing is to
fi nd a compression caused by the mesenteric superior artery
(superior mesenteric artery syndrome or Wilkie´s syndrome)
that has been described associated to several disorders (surgical
interventions (3-4), paraplegia (5), orthopedic surgery (6),
etc). The cases of duodenal compression caused by superior
mesenteric vein are very infrequent and they have been
described as associated to aneurysm of the superior mesenteric
vein (7,8) or to malpositions of such vein (9,10). For the
diagnosis, it is very useful the performance of an abdominal
computed tomography (11) which allow you to study the
relation between the mesenteric vessels and the duodenum, as
well as identify other possible causes of obstruction (12,13).
In the cases published on duodenal compression caused by the
superior mesenteric vein the treatment was surgical. This was
not necessary in our patient due to her good clinical progress
with conservative treatment.
FIGURE LEGEND
Ao: Aorta
D: Third duodenal portion
VM: Superior mesenteric vein
AM: Superior mesenteric artery
Arrow: Duodenal compression caused by the superior mesenteric vein.
REFERENCES
| 1. Ylinen P, Kinnunen J, Hockerstedt
K. Superior mesenteric artery syndrome: a follow-up study of 16 operated patients. J Clin Gastroenterol 1989; 11:386-391 2 Hines JR, Gore RM, Ballantyne GH. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am J Surg 1984; 148:630-632 3. Goes RN, Coy CS, Amaral CA, Fagundes JJ, Medeiros RR. Superior mesenteric artery syndrome as a complication of ileal pouchanal anastomosis. Report of a case. Dis Colon Rectum 1995; 38:543-544 4. Blebea J, Sax HC, Geary KJ, Ouriel K. Superior mesenteric artery syndrome after end-to-side aortofemoral bypass. J Vasc Surg 1990; 11:726-727 5. Wilkinson R, Huang CT. Superior mesenteric artery syndrome in traumatic paraplegia: a case report and literature review. Arch Phys Med Rehabil 2000; 81:991-994 |
6. Shapiro G, Green DW, Fatica NS,
Boachie- Adjei O. Medical complications in scoliosis surgery. Curr Opin Pediatr 2001; 13:36-41 7. Liessi G. Gli aneurismi dellásse spleno-portale e della vena mesenterica superi. Osservazione di quattro casi. Radiol Med 1988; 75:36-39. 8. Mathias KD, Hoffmann J, Krabb HJ, Polonius MJ. Aneurysm of the superior mesenteric vein. Cardiovasc Intervent Radiol 1987; 10:269-271 9. Hecht J, Gruhn C, Schoenberg MH. Vena-mesenterica-superior-Syndrom-eine Duodenalstenose, bedingt durch eine atypisch verlaufende V. Mesenterica superior. Chirurg 2001; 72:186-189. 10. Vejborg IM, Mantoni MY, Nielsen OH. Kongenit duodenal obstruktion forarsaget af abnormt forlobende vena mesenterica superior. Ugeskr Laeger 1990; 152:3012-3013. 11. Konen E, Amitai M, Apter S et al. CT angiography of superior mesenteric artery syndrome. Am J Roentgenol 1998; 171:1279-1281 |
12. Long FR, Mutabagani KH,
Caniano DA, Dumont RC. Duodenum inversum mimicking mesenteric artery syndrome. Pediatr Radiol 1999; 29:602-604 13. Siddiqui MN, Ahmad T, Jaffary A. Retroperitoneal fungal abscess presenting as superior mesenteric artery syndrome. Postgrad Med J 1996; 72:433-444 |