1Michalski Aleksander,
1Gil Dariusz,
1Mazur Włodzimierz,
1Machniak Mariusz,
2Kondera-Anasz Zdzisława,
2Mertas Anna,
3Mazurek Urszula
1. Department of Internal Medicine,
2. Department of Immunology and Serology,
3. Department of Biochemistry and Biophysics,
Medical University of Silesia, Katowice, Poland
Key words:
chronic hepatitis C, interferon alpha-2b,
plasminogen activator inhibitor-1,.
tissue plasminogen activator.
Abbreviations used in article:
IFN, interferon alpha; PAI-1, plasminogen activator
inhibitor-1; TGF beta, transforming growth factor-
beta; t-PA, tissue plasminogen activator
Liver and biliary system
ARCH GASTROENTEROHEPATOL 2007; 26 (No 1-2)12-16
Plasminogen activator
inhibitor-1 and tissue-type
plasminogen activator
changes induced by interferon
alpha in patients with chronic
hepatitis C
ABSTRACT
INTRODUCTION: In healthy subject interferon alpha signifi cantly increased
plasma levels of tissue plasminogen activator and plasminogen activator inhibitor-
1. Aim of this study is to determine the effects of interferon alpha on concentrations
of plasminogen activator inhibitor-1 and tissue plasminogen activator in patients
with chronic viral hepatitis C.
METHODS: Plasma concentration of plasminogen activator inhibitor-1 and tissue
plasminogen activator were measured in 11 patients (IFN group) with chronic
viral hepatitis C after subcutaneous injection of 3 MU of interferon alpha and
in 6 patients with chronic viral hepatitis C after subcutaneous injection of 1ml
0,9%NaCl (Control group). The blood samples were taken before (0) and 1,2,4,6,10
and 24 hours after interferon alpha or placebo injection.
RESULTS. Mean plasma concentrations of plasminogen activator inhibitor-1 in
IFN group rapidly decreased from baseline 53,4 ng/ml to minimum 32ng/ml at 2h
after administration of interferon alpha. There were no changes in plasminogen
activator inhibitor-1 concentration in Control group and in tissue plasminogen
activator concentration in both groups.
CONCLUSION: Decrease of plasma plasminogen activator inhibitor-1
concentration after administrations of interferon alpha probably refl ects interferon
infl uence to plasminogen activator inhibitor-1 synthesis in the liver.
INTRODUCTION
Plasminogen activator inhibitor-1 (PAI-1) is the major
physiological inhibitor of both tissue-type plasminogen
activator (t-PA) and urokinase-type plasminogen activator (u-
PA) and plays an important role in the control of plasminogen
dependent proteolysis (1). Plasminogen activators convert the
inactive plasminogen to active form plasmin. Plasmin plays
a fundamental role in fi brinolysis and another biological
processes with localised proteolysis of the extracellular matrix,
such as tissue remodelling, organogenesis, infl ammation,
tumour invasion and metastasis (2). In these processes plasmin
improves own proteolytic activity and activated matrixdegrading
enzymes.
Increased plasma PAI-1 activity has been detected in
pathological conditions associated with acute phase related
responses. It has been demonstrated that lipopolisacharide,
IL-1 beta and TNF alpha increase PAI-1 plasma levels in rats
(3,4,5,6).
PAI-1 is produced by a variety of cells including: endothelial
cells, hepatocytes, smooth muscle cells, magacaryocytes and
malignant cells (7). The origin of plasma PAI-1 is unknown,
but studies on human tissues showed that plasma PAI-1 is
hepatic and endothelial origin, but unknown is which is the
most important (6, 8). Recent studies revealed that PAI-1 was
produced in human liver after ischaemia reperfusion injury in
patients who underwent partially hepatectomy (9).
Interferon (IFN) alpha is usually used in the treatment in
chronic hepatitis C patients most often with ribavirin. IFN
exerts an antiviral, immunomodulatory, antiproliferative and
antifi brotic activity (10). Fibrosis in the liver leads to the
increased synthesis and accumulation of proteins in extracellular
matrix and this can result in the signifi cant deterioration of liver
function (11). One of the factors which promote fi brogenesis
and can inhibit degradation of extracellular matrix proteins
is transforming growth factor-beta (TGF-beta). TGF beta is
secreted to extracellular matrix in an inactive form, which can
be activated by PAI-PA-plasmin cascade and on the other hand
PAI-synthesis is positively regulated by TGF-beta(12). Castilla
et al.(13) reported that TGF-beta1mRNA was overexpressed
in patients with chronic hepatitis and those who responded
to interferon alpha therapy demonstrated normal hepatic
mRNA cytokine levels following treatment. Tshushima et al.
(14) demonstrated that circulating plasma TGF-beta1 levels
in patients with chronic hepatitis C were reduced at the end
of IFN alpha treatment. Mazur et al. (15) observed decreased
serum TGF beta-1 concentration during IFN-alpha therapy
in patients with chronic viral hepatitis C, both in sustained
and partial responders. Corssmit et al. (16) showed that in
healthy human subjects administration of IFN alpha resulted
in the rapid increase of level of t-PA, PAI-1 antigen as well as
plasminogen activator (PA), PAI-1 activity which decreased
after few hours. Connecting antifi brotic activity of INF with
results of Corssmit’s study and the role of cascade PAI-PAplasmin
in activation of TGF-beta1 we wanted to evaluate the
short-term response of plasma PAI-1 and t-PA antigens after
IFN alpha administration in patients with chronic viral hepatitis
C. As to our knowledge there are no published data on PAI-1
and t-PA responses immediately after IFN administration in
patients with chronic viral hepatitis C.
MATERIAL AND METHODS.
The study was performed as a randomized, single blind,
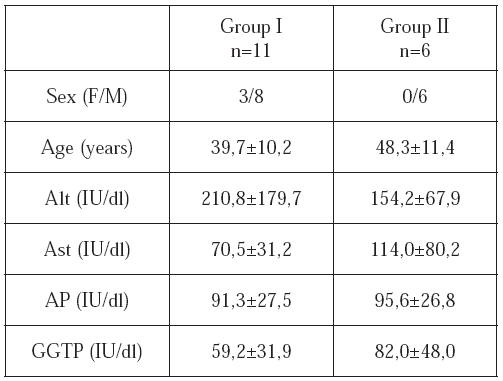
placebo-controlled study in 17 hospitalised patients (14 male,
3 female) with chronic viral hepatitis C. The diagnosis of
chronic viral hepatitis C has been confi rmed by liver biopsy,
clinical data and results of laboratory tests (Tab.1). Anti-
HCV antibodies (third generation test) and HCV-RNA (PCR
method) in sera were positive in all patients for minimum 6
months period before including to the study. Patients with
co-infection with hepatitis B virus, autoimmune hepatitis,
coagulation abnormalities, history of alcohol abuse or drug
related disease were excluded. The patients were divided
into two groups. 3 MU of interferon alpha-2b (Intron A,
Schering-Plough) were given to 11 patients (IFN group).
Equivalent volume of isotonic saline was administered to 6
patients (Control group). After that all patients were treated
with IFN and ribavirin according to standard protocol. Blood
samples were taken before (t-0= 08.00am) and 1,2,4,6,10,24
hours after administration of IFN alpha or isotonic saline
solution. Blood was collected by separate venipunctures from
the antecubital vein with appropriate amount of anticoagulant
(3.8% natrium citrate in proportion 9:1). Plasma samples
were obtained by 30-min. centrifugation at 2000xg at 4 0C
and were immediately frozen and stored at –70 0C. Plasma
concentrations of PAI-1 and t-PA were measured by ELISA
method (American Diagnostics, USA). Results are expressed
as ng per ml and presented as mean ± SD.
Differences within groups were tested by analysis of
ANOVA and Fisher’s LSD test, data between groups were
tested by the Student’s t-test. A value p<0,05 was considered
to represent statistical signifi cance. The study was approved
by the Local Medical Ethical Commitee.
RESULTS.
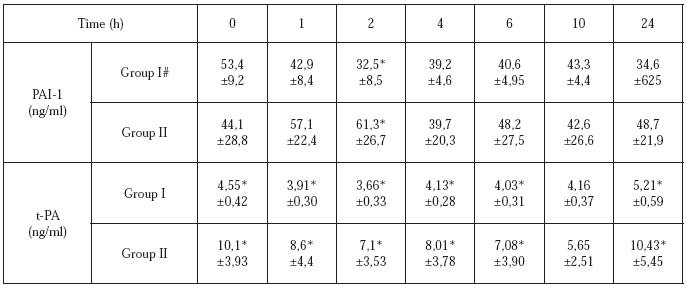
Elevated plasma concentrations of the PAI-1 were found
in 12 subjects (11 in IFN group I and 1 in Control group),
differences however were not statistically signifi cant. Plasma
concentrations of the t-PA were normal in all patients of Group
I, except one (Tab.2). In IFN and Control group concentrations
of t-PA antigen at fi rst decreased (IFN group, t=2h; Control
group, t=10h) and afterwards increased but these changes were
not signifi cant (Tab.2). Mean plasma concentrations of PAI-
1 in IFN group rapidly decreased from baseline 53,4 ng/ml
to minimum 32ng/ml at 2h after administration of IFN alpha
(LSD test p<0,001) and were double lower when compared
with Control group (t-test p<0,005). This profi le changes of
PAI-1 were observed in all patients in IFN group and were
signifi cant (ANOVA p<0,005). In Control group we did not
observe these changes (Table 2).
DISCUSSION.
Results of plasma concentrations of PAI-1 in patients
with liver disease were unequivocal. Most of the studies were
performed in patients with advanced liver disease. Similarly to
our results Takahashi et al. (17) showed increased PAI-1 plasma
concentrations in subjects with chronic hepatitis. Inuzuka et
al. (18) observed that increased PAI-1 plasma concentrations
correlated with stage of liver fi brosis. In our study patients
with elevated plasma concentrations of PAI-1 were classifi ed
to fi brosis score 1-2 according to Sheuer classifi cation, thus
they had no advanced liver fi brosis. Corssmit et al. (16) showed
that in healthy human subjects administration recombinant
IFN alpha signifi cantly increased plasma levels of t-PA, u-PA
and PAI-1 after 6 to 12 hours. We could not consolidate these
fi ndings. Corssmit et al. (16) suggested that these changes
were connected with action of IFN alpha on endothelial cells
but this did not cause alternations in generation of plasmin
and thrombin thus function of haemostasis and fi brinolysis
were not impaired. In vitro effect of IFN alpha on fi brinolysis
showed unequivocal results (16, 19). Increased concentration
of u-PA and decreased release of PAI-1 as well as a reduction
of plasminogen activators (t-PA, u-PA) activity and increased
levels of PAI-1 were reported (16, 19). Hayashi et al. (20)
found no signifi cant differences in plasma PAI-1 level in
patients with chronic viral hepatitis C before and after IFN
treatment for 14 consecutive days. Our study showed that after
single injection of IFN alpha plasma concentration of PAI-1
rapidly and signifi cantly decreased and remained low up to
24 hours.
In healthy subjects diurnal variations of plasma
concentrations of PAI-1 have been observed. The highest
concentrations have been found between 8 a.m. to 10 a.m.
and the lowest once at 3 p.m. (21). Changes of plasma PAI-1
concentrations in ours patients didn’t refl ect this normal diurnal
pattern (healthy subject were not observed in our study).
Animal studies have suggested that PAI-1 is important in the
liver response to injury; for example partial hepatectomy or
subcutaneous injection of bacterial lipopolysacharide resulted
in elevation of PAI-1 mRNA concentration in liver (22).
Inoue et al. (9) showed elevated PAI-1 synthesis in human
liver after ischaemic reperfusion injury provoked by Pringle’s
manoeuvre and demonstrated signifi cant correlation between
activity of PAI-1 and TGF beta-1. It was demonstrated that
synthesis of PAI-1 in hepatoma and endothelial cells was
induced by IL-1, TNF and endotoxins (8, 23, 24) and that
synthesis of PAI-1 by hepatoma cells, hepatocytes and hepatic
stellate cells was regulated by TGB beta-1 (5, 8). Mazur et
al. (15) observed decreased serum TGF beta-1 concentration
during IFN-alpha therapy in patients with chronic viral
hepatitis C, both in sustained and partial responders. Thus it
seems probable that plasma PAI-1 concentration could refl ect
the degree of liver injury. It is also possible that decrease of
plasma PAI-1 concentration following administration of IFN
alpha may be connected with its impaired synthesis by liver
cells. Bueno et al. (25) showed, that administration of IFN
resulted in decrease of PAI-1 immunoreactivity in liver tissue
and PAI-1 activity in non-parenchymal liver cells extracts. In
our patients plasma concentrations of PAI-1 did not correlate
with changes of plasma concentration of t-PA which is mainly
synthesised by endothelial cells. So it is possible that PAI-1
plasma concentrations changes and the lack of alteration in
t-PA plasma concentrations after administration of IFN are not
associated with INF infl uence to the endothelial cells.
CONCLUSIONS
Decrease of plasma PAI-1 concentration after
administrations of IFN probably refl ects interferon infl uence
to PAI-1 synthesis in liver.
Table 1. Clinical data and laboratory results of patients (mean ± SD)
Table 2. Plasma PAI-1 and t-PA concentrations (mean±SD)
REFERENCES
| 1. Loskutoff D, Sawdey M, Mimuro J. Plasminogen activator inhibitor type-1. Prog Hemost Thromb 1989; 9: 87-115. 2. Saksela 0, Rifkin D. Cell associated plasminogen activation: regulation and physiologic functions. Annu Rev Cell Biol 1988; 4: 93-126. 3. Podor TJ, Hirsh J, Gelehrter TD et al. Type 1 plasminogen activator inhibitor is not an acute phase reactant in rats. Lack of IL-6 and hepatocyte-dependent synthesis. J Immunol 1993; 150: 225-35. 4. de Boer JP, Abbink JJ, Brouwer MC et al. PAI-1 synthesis in the human hepatoma cell line HepG2 is increased by cytokines - evidence that the liver contributes to acute phase behaviour of PAI-1. Thromb Haemost 1991; 65: 181-185. 5. Busso N, Nicodeme E, Chesne Ch et al. Urokinase and type I plasminogen activator inhibitor production by normal human hepatocytes: modulation by infl ammatory agents. Hepatology 1994; 20: 186-190. 6.Chomiki N., Henry M., Alessi MC., Anfosso F., Juhan VI. Plasminogen activator inhibitor- 1 expression in human liver and healthy or atherosclerotic vessel walls. Thromb Haemost 1994; 72: 44¬-53. 7.Simpson AJ, Booth NA, Moore NR, Bennett B. Distribution of plasminogen activator inhibitor (PAI-1) in tissues. J Clin Pathol 1991; 44:139- 143. 8.Knittel T, Fellmer P, Ramadori G. Gene expression and regulation of plasminogen activator inhibitor type 1 in hepatic stellate cells of rat liver. Gastroenterology 1996; 111: 745-754. 9. Inoue K, Sygawara Y, Kubota K, Tadatoshi T, Makuuchi M. Induction of type 1 plasminogen activator inhibitor in human liver ischemia and reperfusion. J Hepatol 2000; 33: 407-414. |
10. Pestka S, Langer T, Zoon K.
Interferons and their actions. Annu Rev Biochem 1987, 56: 727- 777. 11. Friedman SL. The cellular basis of hepatis fi brosis. N Eng J Med 1993, 328: 1828-1835. 12. Lyons R, Gentry L, Purchio A, Moses H. Mechanism of activation of latent recombinant transforming growth factor β1 by plasmin. J Cell Biol 1990; 110: 1361-1367. 13. Castilla A, Prieto J, Fausto N. Transforming growth factor beta 1 in chronic liver disease: effects of interferon alfa therapy. N Eng J Med 1991; 324: 933-940. 14. Tshushima H, Kawata S, Tamura S et al. Reduced plasma transforming growth factorbeta1 levels in patients with chronic hepatitis C after interferon alpha therapy: association with regression of hepatic fi brosis. J Hepatol 1999; 30: 1-7. 15. Mazur W, Braczkowski R, Gonciarz M et al. Fibrosis TGF-β1 marker in blood of chronic hepatitis C patients during interferon alfa-2B therapy. Med. Sci Monit 1999; 5 (Suppl.1): 73-76. 16. Corssmit E, Levi M, Hack C. Fibrinolytic response to interferon-α in healthy human subjects. Thromb Haemost 1996; 75: 113-117. 17. Takahashi H, Tatewaki W, Wada K, Niwano H, Shibata A. Fibrinolysis and fi brinogenolysis in liver disease. Am J Hematolog 1990; 34: 241- 245. 18. Inuzuka S, Ueno T, Torimura T. The signifi cance of colocalization of plasminogen activator inhibitor-1 and vitronectin in hepatic fi brosis. Scand J Gastroenterol 1997; 32: 1052-1060. 19. Smith TJ, Ahmed A, Hogg MG, Higgins PJ. Interferon is an inducer of plasminogen activator type 1 in human orbital fi broblasts. Am J Physiol1992; 263: C24-C29. |
20. Hayashi T, Ro S,
Kamogawa A et al. Changes in plasma tissue plasminogen activator (t-PA) and plasminogen inhibitor 1 (PAI-1) by the i nterferon treatment for chronic hepatitis C. Rinsho Byori 1995; 43: 948-952. 21. Piscaglia F, Siringo S, Hermida RC et al. Diurnal changes of fi brinolysis in patients with liver cirrhosis and esophageal varices. Hepatology 2000; 31: 349-357. 22. Schneiderman J, Sawdey M, Craig H, Thinnes T, Bordin G, Loskutoff DJ. Type 1 plasminogen activator inhibitor gene expression following partial hepatectomy. Am J Pathol 1993: 143: 753-7¬62. 23. Loskutoff DJ, Sawdey M, Keeton M, Schneiderman J. Regulation of PAI-1 gene expression in vivo. Thromb Haemost 1993; 70: 135-137. 24. Quax P, van den Hogen C, Verheijen J et al. Endotoxin induction of plasminogen activator and plasminogen activator inhibitor type I mRNA in rat tissues in vivo. J Biol Chem 1990; 265: 15560-15563. 25. Bueno MR, Daneri A, Armendariz-Borunda J. Cholestasis-induced fi brosis is reduced by interferon alpha-2a and is associated with elevated liver metalloprotease activity. J Hepatol |