|
|
Alimentary
tract and pancreas Alimentarni
trakt i pankreas |
||
|
1 Institute for Infectious and Tropical Diseases, Clinical Center of Serbia, Medical Faculty University of Belgrade 2 Department for Infectious Diseases, General Hospital of U`ice 3 Medical Faculty University of Belgrade. |
ARCH
GASTROENTEROHEPATOL 2003; 22 (No 1 - 2): 12 – 17 Epidemiological
and clinical data
of outpatients with chronic
viral hepatitis Epidemiolo{ko-klini~ki
podaci ambulantnih bolesnika
sa hroni~nim virusnim hepatitisom (
accepted May 29th, 2003 ) |
||
|
Key
Words: chronic
hepatitis, Hepatitis
C Virus, Hepatitis
B Virus |
Abstract Total
of 212 outpatients with chronic hepatitis were evaluated. Patients were
followed-up at lest six months
to two years. Clinical, laboratory, ultrasonography examination and viral
serological tests were performed
for differential diagnosis. Viral infection was discovered in 179 patients (Hepatitis
C Virus, Hepatitis
B Virus, and co-infection with both viruses in 122, 56 and 1
patients, respectively). Distribution by
age confirmed more numerous young patients (from 21-30 years) in chronic
hepatitis C, while majority of
patients with chronic hepatitis B, were older (from 41-50 years). The higher
prevalence of male gender
was in both groups. Epidemiological data were positive in about half of
patients with chronic C hepatitis,
while majority of patients with chronic hepatitis B were without known route
of infection. Most
patients with chronic hepatitis C were recognized as intravenous drug abusers
(48%). Analyzed alanine
aminotransferase values confirmed mild elevation in the majority of patients
(45.28%), independent of
etiology. The most frequent associated disease in both groups was fatty liver
of unknown cause.
Clinically, investigated patients were mostly presented as mild chronic liver
disease, exceptionally, with
liver cirrhosis. In
conclusion, majorities of outpatients are young males with Hepatitis
C Virus infection, mostly drug abusers.
Histology assessment of liver tissue would yield more information on
differential diagnosis, eventually
associated disease, and stage of fibrosis that is crucial for disease
progression. Sa`etak Ispitano
je ukupno 212 ambulantnih bolesnika sa hroni~nim hepatitisom. Bolesnici su
pra}eni od {est meseci do dve
godine. Radi diferencijalne dijagnostike, ura|ena su klini~ka i
laboratorijska ispitivanja, pregled ultrazvukom
kao i virusolo{ki serolo{ki testovi. Virusna infekcija je na|ena u 179
bolesnika (hepatitis C virus: 122, hepatitis
B virus: 56, konfekcija sa oba virusa :1). U odnosu na uzrast, u
bolesnika sa hroni~nim C
hepatitisom najbrojnijie su bile mla|e osobae (od 21-30 godina), dok je
ve}ina bolesnika sa hroni~nim B
hepatitsom bila starija (od 41-50 godina). U obe grupe bolesnika dominirali
su mu{karci. Pozitivne epidemiolo{ ke
podatke je imalo oko polovine bolesnika sa hroni~nim C hepatitisom. Ve}ina
bolesnika sa hroni~nim
B hepatitisom nije imala podatke o na~inu zaraze. Intravenski narkomani su
bili najbrojniji me|u
bolesnicima sa hroni~nim C hepatitisom (48%). Vrednosti alanin
aminotransferaze su bile umereno povi{ene
u ve}ine bolesnika (45.8%), nezavisno od etiologije. Od udru`enih bolesti,
masna jetra neprepoznatog uzroka
je bila naj~e{}i nalaz u obe grupe bolesnika. Ve}ina bolesnika je imala bla`i
klini~ki oblik, ciroza
jetre je bila retka. U zaklju~ku, najbrojnije ambulante bolesnike ~ine osobe
sa hroni~nim C hepatitisom, uglavnom
mla|eg uzrasta i epidemiolo{kim podacima o intravenskom konzumiranju droge. Histolo{ka
procena tkiva jetre bila bi zna~ajna radi detaljnije diferencijalne
dijagnoze, otkrivanja eventualnih drugih
stanja i odre|ivanja stadijuma fibroze kao najzna~ajnijeg faktora za progresiju
bolesti. |
||
|
Klju~ne
re~i: hroni~ni
virusni hepatitis, Hepatitis
C Virus, Hepatitis
B Virus |
|||
|
|
INTRODUCTION Chronic
viral hepatitis (CVH) is a global public health problem.
Two primarily hepatotropic viruses, Hepatitis C virus
(HCV) and hepatitis B virus (HBV),
are main causes of the
disease. It is estimated that approximately 400 million, and
up to 200 million of individuals in the world, suffer from chronic
viral B and C infections, respectively (1,2). Viral transmission
is mainly parenteral, sexual and perinatal. Other
ways of transmission (percutaneous and nosocomial), occur
as well (3-7). Fortunately, rigorous screening practices diminished
the risk of transmission through blood transfusion. The
pathogenesis of CVH is still unclear. Replicating in hepatocytes,
viruses are capable to produce persistent infection and
as a consequence, chronic inflammation of the liver. Liver
damage mainly stems from cellular immune response, but
many other factors can influence its clinical presentation and
final outcome (8,9). Alcohol use, male sex, age at disease acquisition,
co-infection with HBV and HIV,
genetic background,
metabolic diseases (type II diabetes mellitus, hyperlipidemia,
iron overload), high body weight, even smoking,
etc., are associated with more rapid disease progression, particularly
in chronic hepatitis C (CH-C) (10-19). Clinical
course of CVH can be extremely various and is nonpredictable. It
may have a wide spectrum of features, ranging from
non-symptomatic to severe hepatitis ending to liver cirrhosis,
or even, hepatocellular carcinoma (HCC) (20-22). Efforts
to discover infection, understanding clinical manifestations and
natural history of the disease, careful monitoring of
patients, and eventually, offering antiviral therapy, are
critical to prevent progression of the disease and its serious sequelae. AIM
OF STUDY The
aim of this study was to investigate some of epidemiological and
clinical data of outpatients in order to characterize
them as a particular group of patients with chronic
viral hepatitis. Study objectives were following: -
Estimate the etiology of chronic viral hepatitis in outpatients -
Analyze demographic data of patients comparing with aetiology -
Identify the route of viral transmission and the risk of infection -
Notice other diseases as co-factors that could be important for
the disease progression -
Interpret the results of ALT values as a parameter for liver
necrosis -
Evaluate the stage of the disease on the basis of clinical picture
and radiological imaging PATIENTS
AND METHODS Total
of 212 outpatients with chronic liver disease (138 males,
74 females; age range: 13-76 years) was randomly included
in this investigation from January 2000 to December
2001. Patients were followed-up at Hepatology Clinic
at least six months to fulfill criteria of chronic hepatitis. Participants
were pending for liver biopsy, although some of
them refused it or had relative or absolute contraindications. They
were not hospitalized, nor received antiviral therapy before
the investigation. All analyzed parameters were taken
retrospectively, including demographic data, behavioral and
other risk of infection, alcohol or drug consumption, symptoms
of the disease, and clinical findings. As well, routine laboratory
analyzes (glucose, nitrogen, blood count, lipids,
etc.), liver function tests: alanine aminotransferase (ALT),
albumin, PT, PTT etc., and ultrasonography findings of
the upper abdomen, were performed. For differential diagnosis of
chronic or other liver diseases (hereditary metabolic diseases,
autoimmune hepatitis, liver cancer, etc.), selected tests
(ceruloplasmin, alpha 1 antitripsin, autoantibodies etc.), and
tumor markers (AFP and CEA), were done. Patients suspected for
liver or other malignancy were excluded from the study.
Serological tests for HBV, HCV,
and HIV markers were done
by third generation enzyme-linked immunosorbent assay
(ELISA) with commercial kits. Positive anti HCV
sera was confirmed
using recombinant immunoblot assay (RIBA). Statistical
analysis was done for parametric and non-parametric data
(Student's t test, x2
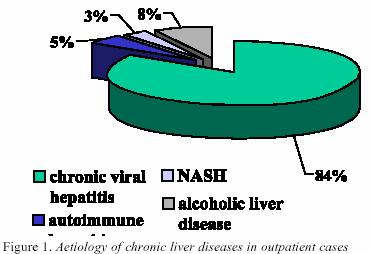
test). A p<0.05 was considered significant. RESULTS 1.
Aetiology of chronic liver disease The
etiology of chronic liver disease is shown in Figure 1. The
majority of 212 studied patients had chronic viral hepatitis
(84%) (DF=5; x2
=300.2;p<0.01). Autoimmune
hepatitis, alcoholic liver disease and nonalcoholic liver
steatosis/steatohepatitis (mainly caused by type
II diabetes mellitus and hypelipidemia), were other discovered diseases,
but in a significant lower number of patients.
Liver steatosis or steatohepatitis were defined by ultrasonography
finding of fatty liver depending on presence of
ALT elevation. 2.
Aetiology of chronic viral hepatitis Among
of 179 patients with chronic viral hepatitis, mostly (122/179;
68%) of them had HCV infection.
A significant lower
number (56/179; 31%) of patients had chronic B hepatitis
(DF=5; x2
=300.1;p<0.01). One patient
had dual infection with both viruses.
3.
Gender of patients with chronic viral hepatitis The
overall prevalence of male gender in total number of
patients with chronic viral hepatitis was significantly higher
in males: 64% than females: 36% DF=1;x2=0.11;p<0.05). Prevalence
of male gender was also significantly higher in
each group of patients with CH-C (DF=1; x2=8.5; p<0.01),
and CH-B (DF=1; x2=5.8;p<0.05). 4.
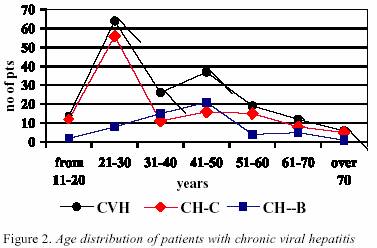
Age of patients with chronic viral hepatitis Age
distribution by etiology in patients with chronic viral
hepatitis is shown in Figure 2. Mean
age of patients with chronic viral hepatitis was 38 years
(8=38.6;SD=14.8). Group of patients aged from 21- 30
years was most frequent (DF=6; x2=87.8;p<0.01).
Age of
patients with CH-C were from 13-76 years (8C=35.8; SD=15.7),
while patients with CH-B were aged from 17-71 years
(8B=41.5;SD=12.9).
Analyzing
age by etiology of CVH, significant difference was
noticed between patients with CH-C and CH-B; patients
with CH-C were significantly younger than patients
with CH-B (DF=6; x2
=33.3;p<0.01). Group
of patients aged from 21-30 years was the most frequent
in CH-C, while in CH-B, the most frequent group included
patients from 41-50 years (DFC=6;
x2=94.5;p<0.01; DFB=6; x2=41;p<0.01). 5.
Epidemiological data of patients a.
The overall prevalence of positive (73/122) and negative (49/122)
epidemiological data was similar in CH-C patients
(DF=1; x2
=4;p>0.05). In contrast, the majority of patients
(13/56) with CH-B had no epidemiological data of infection
(DF=14; x2=14;p<
0.01). Patient
with dual HCV and HBV
infection had no data about
its risk.
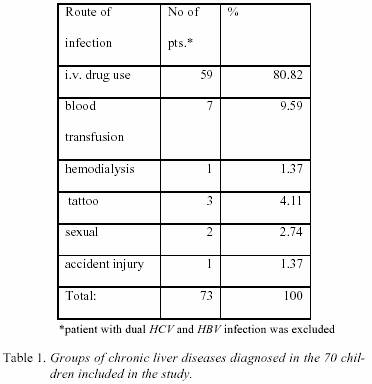
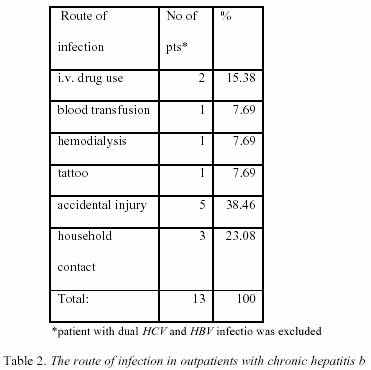
b.
Patients with positive epidemiologal data were further analyzed
in details about the route of infection and the results
are shown in Table 1., and Table 2. The
majority of patients with CH-C had history data about
i.v. drug use (80%) (DF=5; x2
=198.8;p<0.01). In total
number of patients with CH-C, i.v. drug users were 48.36%. Seven
out of 73 patients received blood transfusion, other
routes of infection were less found. Among
patients with CH-B, 5/13 were infected by accidental injury.
All patients were healthcare workers, three of them
were dentists. Household contacts with infected person were
noticed in three patients.
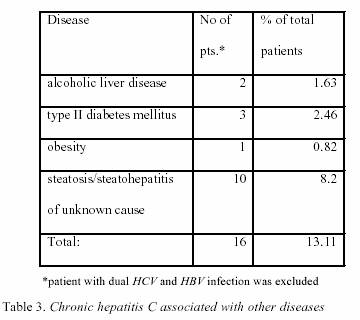
6.
Co-morbidity of chronic viral hepatitis with other diseases Investigations
of patients history, clinical and biochemical data,
and ultrasonography findings, revealed other diseases shown
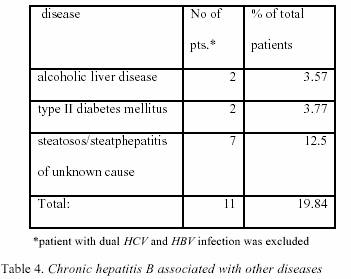
in Table 3., and Table 4. The
most common finding of associated disease in patients
with CH-C was unknown caused liver steatosis/steatohepatitis
(10/16, or 8% of total patients with
CH-C) (DF=3; x2=2.77;p>0.05). Steatosis/steatohepatitis
of unknown cause was also the most
frequent finding in patients with CH-B (7/11 or 12% of
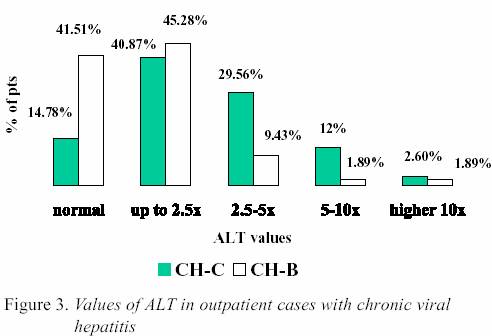
total patients with CH-B). 7.
Values of alanine aminotransferase in patients with chronic
viral hepatitis Values
of alanine aminotransfere were divided in 5 groups:
normal value, up to 2.5x, from 2.5-5x, from 5-10x, and
10x upper limit than normal value, respectively. The
results of ALT values are shown in Figure 3. 8.
Viral hepatitis Mild
elevation of ALT values (from normal-2.5x upper limit
of normal value), were noticed significantly most frequent in total
number of patients (45.28%) (DF=5;
x2=21.7;p<0.01). As
well, mild elevation of ALT values was most frequent in
the majority in each group of patients (CH-C: DF=4;
x2 =5.8; p<0.01) (CH-B: DF=4; x2=45.8;p<0.01). Comparing
etiology and ALT values, significant higher values
of ALT were noticed in patients with CH-C then in CH-B
patients (DF=5; x2
=16.7; p<0.01). Persistently
normal ALT values were defined by at least 3
determinations within screening period of 6 months or longer.
Normal values of ALT were found in 17/115 (14.78%%),
and 22/53 (41.51%) in CH-C and CH-B patients,
respectively. In CH-C patients, younger aged group
(from 20-31 years) was sifnificantly higher than
other
groups. (DF=5; x2=20.7;p<0.01).
In this group of patients,
CH-C patients, there was no difference between gender
(DF=9; x2
=0;p>0.05). In
CH-C patients with normal ALT values, positive antibodies
to HCV confirmed the diagnosis. HCV RNA was
not determined. In CH-B patients, HBeAg was done in 6/22
patients, and was negative. Analyzed
ALT values in CH-C patients with associated other
diseases did not show any significant difference (DF=3;
x2=2.77;p>0.05). 9.
Clinical features of patients with chronic viral hepatitis Evaluation
of clinical, biochemical and ultrasonography findings
of patients with chronic viral hepatitis confirmed that
mostly of them had chronic hepatitis without liver
cirrhosis (CH-C: 94%, CH-B: 93%). DISCUSSION Chronic
liver disease has different aspects. Patients usually
have no symptoms until liver cirrhosis and its complications developed.
Elevated aminotransferase values, often
at routine laboratory examination, usually take them to
hepatology units for evaluating possible liver disease. One
of the most important assignments for hepatologist is to
make correct differential diagnosis in order to recognize disease,
cure it with adequate therapy, and prevent its serious outcome.
Moreover, particular problem in outpatients were
wide spectrum of laboratory testings, careful clinical examination,
detailed history taking and epidemiological data,
and if necessary, additional radiological imaging that must
be done. Our
study was conducted in Hepatology Clinic which prime
purpose is in diagnosing and following-up patients with
infectious diseases. Exclusion or confirmation viral aetiology
in the spectrum of other chronic liver disease is the
first step for many general practitioners or gastroenterologists. From
diverse laboratories, blood transfusion units,
hemodialysis centers and phsyhiatric departments, patients
with positive hepatitis viruses are directed to visit our
Clinic for further clinical examination. Because of that, the
results of our investigation in two-year period strengthened the
fact that majority of outpatients (84%) have chronic
viral hepatitis, exclusively caused by HCV
and HBV.
Our study discovers more number of patients with chronic
HCV infection (84%) than CH-B, which is
also, general
epidemiological trend in other countries in the last decade
(1). Because of the similar transmission route, it was
expected a possible co-infection with both viruses and we
noticed it, but only in one patient. This
investigation confirms that males (64%) suffer from
CVH more than females, independently on aetiology. Past
data from the literature and our experience that persistence of HBV
is more often in males, are not completely resolved
until now. Some incomplete explanation was given
through interfering of hormones and viral replication. Recently
published epidemiological studies of HCV also
confirmed more inclination of males to become long term
carriers, after discovering that young females could eradicate
the virus up to 50% (23). At the same time, in our socioeconomic
milieu, males are more liable for behavioral risks
such as drug abuse and promiscuity what is critical for
percutaneous and sexual infection with both viruses. Intravenous
drug use has replaced blood transfusion as the
most common route of transmission of HCV. Approximately
90% of drug users after 5 years become infected
(24,25). Such drug use accounts for around two thirds
of HCV infections in U.S., and other developed countries.
As it was expected in our study, in CH-C, more frequent
patients were males, younger age (from 20-31 years)
and drug users (49%). On the contrary, majorities of patients
with CH-B had no data about infection and were older
than CH-C patients. Drug abuse as an epidemiological risk
is confirmed only in 15% of these patients. Interesting
data is that only one patient with CH-C (lower than
1% of total patients), was infected through hemodialysis. According
to data from several dialysis departments in
our country, almost 80% patients are infected with HCV (Dr.
S. Zerjav, personal communication). It
is worth to stress that among CH-B patients, 8/56 (14%)
were infected through accidental injury or household contacts.
This data requires use of preventive vaccination measures
of all healthcare workers and persons living with
infected patients, including sexual partners and other
relatives (26,27). The
specific factors that lead to progression of CVH are still
unclear. Investigation of associated diseases in our patients
discovered few patients with chronic consummation of
alcohol, type II diabetes mellitus and body overweight. But,
most frequent finding in our study was unknown
caused fatty liver estimated by ultrasonography. It
is almost equally presented in CH-C and CH-B (8% and 12%,
respectively), although that is more typical for CH-C (28,29).
It is notified that steatosis in CH-C can be conspicuous in
up to 60% by liver biopsy, induced by metabolic disturbances,
mainly diabetes mellitus type II and obesity.
Virus itself can be also a cause for fatty infiltration, particularly
in genotype 3, when its core and nonstructural part
of the genome (NS5A), disrupt intracellular uptake and
transport of lipids. However, only ultrasonography examination
is not complete for evaluation of fatty infiltration, especially
because of the fact that liver fibrosis can be expressed
as liver steatosis. Liver biopsy, what was not done
in our patients, certainly would be better to estimate and
differentiate this finding. Clinically,
CHV characterizes the insidious nature of the
disease and ALT values may be normal or fluctuate over
its course. Generally, mainly of patients have mild elevation
of ALT as it was noticed in our study (45%). In HCV
infection, extremely high values of ALT (more than 5-10
x upper limit of normal), can be found rarely, does not correlate
with disease progression or viral replication, even in
an acute hepatitis (20-22). During the course of CH-B, after
several years of infection, HBe antigen seroconversion is
followed with high elevation of ALT values in approximately
one third of patients. After that e.g. "elimination" phase,
the later course of the disease is relative benign
and is defined as "inactive". (30,31). "Inactive" disease could
explain lower activity of ALT values in CH-B, especially,
because of older age of patients. Another possibility could
be a high prevalence of drug users in CH-C in our
study, and combined toxic and viral effects on liver necrosis.
In addition, active drug use could explain that lower
prevalence of normal ALT values (14%), what was found
in other studies (approximately 30 %). Otherwise, normal
ALT values are found mostly in younger patients (aged
from 21-30 years), and without difference in gender. That
is in contrast to literature data that population with normal
ALT has distinct features, with inverted male to female
ratio and with no difference in age (32,33). As we had
not possibility to detect HCV RNA in outpatients, it is difficult
to differentiate if positive anti HCV antibodies in these
patients means present or, eventually past infection (34).
As well, in CH-B patients with normal ALT values, we
confirmed negativity of HBe antigen in 6/22 patients. Comparing
ALT values in CH-C patients associated with
other diseases that can accelerate progression of the disease,
we did not find a significant difference, and can not
conclude that this laboratory parameter, without histopatological
finding could be a "surrogate" markers for liver
necrosis and consecutive fibrosis (35-37). The
result that clinical feature of our patients was mainly without
cirrhosis (more than 90%), is explained by the fact
that patients with end stage of liver disease usually need
an intensive hospital care. Possible serious complications not
allowed these patients to be followed-up in the Clinic
for a long period. In
conclusion, the outpatients with chronic hepatitis in Hepatology
Clinic characterized viral infection, mainly with
HCV, and mild clinical features. High-risk populations are
young males, particularly drug users. Beside biochemical, clinical
and radiological imagining data, histopathological
examination is necessary for complete evaluation
of the disease. It can estimate possible associated disease
and stage of fibrosis that is most competent factor for
evaluation of disease progression. |
||
|
|
REFERENCES: 1.
National Institutes of
Health Consensus Development Conference Statement: Management of Hepatitis C: 2002, June
10-12, 2002, Hepatology 2002; 36 (Suppl. 1):
S3-S19. 2.
Alter
M: Epidemiology of hepatitis B in Europe and worldwide. EASL Intern Consensus Conference on Hepatitis B. Program and Manuscripts, Geneva 13-14 Septembar,
2002: 73- 83. 3.
Brook
MG: Sexually acquired hepatitis. Sex Transm Infect 2002; 78: 235-40. 4.
Edlin
BR: Prevention and Treatment of Hepatitis C in Injection Drug Users. Hepatology
2002; 36: S210-219. 5.
Hagan
H, McGough JP, Thiede H et al: Syringe exchange and risk of infection with
hepatitis B and C viruses. Am J Epidemiol 1999;
149: 203- 13. 6.
Arai
Y, Noda K, Enomoto N et al: A
prospective study of hepatitis C virus infection
after needlestick accidents. Liver 1996; 16: 331-4. 7.
Zanetti
AR, Tanzi E, Newell ML: Mother-to-infant transmission of hepatitis C virus. J
Hepatol 1999; 31(Suppl 1): 96-100. 8.
Cerny
A, Chisari FV: Pathogenesis of chronic hepatitis C: immunological features of
hepatic injury and viral persistence.
Hepatology 1999; 30: 595-601. 9.
Walsh
K, Alexander GJM: Update on chronic viral hepatitis. Postgrad Med J 2001;
77: 498-50. 10.
Poynard
T, Ratziu V, Charlotte F et al: Rates and risk factors of liver fibrosis
progression in patients with chronic hepatitis C. J Hepatology
2001; 34: 730-9. 11.
Wong
V, Caronia S, Wight D et al: Importance
of age in chronic hepatitis C virus
infection. J Viral Hepat 1997; 4: 255-64. 12.
Negro
F: Hepatitis C Virus and Liver Steatosis:
Is It the Virus? Yes It Is, but Not
Always. Hepatology 2002; 36: 1050-2. 13.
Wiley
TE, McCarthy M, Breidi L, Layden TJ: Impact of alcohol on the histological
and clinical progression of hepatitis C infection.
Hepatology 1998; 28: 805-9. 14.
-Caronia
S, Taylor K, Pagliaro L et al: Further evidence for an association between
non-insulin dependent diabetes mellitus and chronic
hepatitis C virus infection. Hepatology 1999; 30:
1059-63. 15.
Renou
C, Halfon P, Pol S et al: Histological
features and HLA class II alleles in hepatitis C
virus chronically infected patients with
persistently normal alanine aminotransferase levels. Gut
2002; |
51: 585-90. 16.
Kuzushita
N, Hayashi N, Maribe T et al: Influence of HLA haplotypes on the clinical
course of individuals infected with hepatitis C virus. Hepatology 1998; 27: 240-4. 17.
Mori
M, Hari M, Wada I et al: Prospective study of hepatitis B and C viral infections,
cigarette smoking, alcohol consumption and other
factors associated with hepatocellular
carcinoma risk in Japan. Am J Epidemiol 2000; 151: 131-9. 18.
Pessione
F, Ramond M-J, Njapoum C et al: Cigarette smoking and hepatic lesions
in patients with chronic hepatitis C. Hepatology 2001;34:121-5. 19.
Mohsen
AH, P J Easterbrook PJ, C Taylor C et al: Impact of human immunodeficiency virus
(HIV) infection on the progression of liver
fibrosis in hepatitis C virus infected patients.
Gut 2003; 52: 1035-40. 20.
Sherlock
S, Dooley J. Chronic hepatitis. In: Diseases of the Liver and Biliary
System. Sherlock D, Dolley J (eds). 10 th ed.
London, UK: Blackwell Science Ltd, 1997; 303-37. 21.
Dove
LM, Wright TL: Chronic viral hepatitis. In: Fridman LS, Keef EB. Handbook of liver
disease. Fridman LS, Keef EB (eds). Edimburgh
UK: Churchill Livingstone, 1998: 47-63. 22.
Niederau
C, Lange S, Heintges T et al: Prognosis of hepatitis C: results of a large
prospective cohort study. Hepatology 1998; 28: 1710-2. 23.
.Alter HJ: Hepatology
highlights, Hepatology 2002; 36: 778-80. 24.
Thorpe
LE, Ouellet LJ, Hershow R et al: Risk of hepatitis C virus infection among young
adult injection drug users who share
injection equipment. Am J Epidemiol 2002; 155: 645-53. 25.
Hope
VD, Judd A, Hickman M et al: Prevalence of hepatitis C virus in current
injecting drug users in England and Wales: is harm reduction
working? Am J Public Health 2001; 91: 38-42. 26.
Roggendorf
M, Viazov S. Health care workers and hepatitis B: EASL Intern Consensus
Conference on Hepatitis B. Program and
Manuscripts, Geneva 13-14 Septembar 2002: 121-6. 27.
Van
Steenbergen JE, Working Group Vaccination High-risk Groups Hepatitis B for The Netherlands: Results of an
enhanced-outreach programme of hepatitis B vaccination in
the Netherlands (1998-2000) among men who
have sex with men, hard drug users, sex
workers and heterosexual persons with multiple
partners. J Hepatol 2002, 37: 507-13. 28.
Castéra
L, Hézode C, Roudot-Thoraval F et al: Worsening of steatosis is an
independent factor of |
fibrosis progression in untreated
patients with chronic hepatitis C and paired liver
biopsies, Gut 2003; 52: 288-92. 29.
Rubbia-Brandt
L, Qaudri R, Abid K et al: Hepatocyte steatosis is a cytopathic
effect of hepatitis C virus genotype 3. J
Hepatology 2000; 33: 106-15. 30.
Yuen
MF, Yuan HJ, Hui CK et al: A large
population study of spontaneous HBeAg
seroconversion and acute exacerbation of chronic
hepatitis B infection: implications for antiviral
therapy. Gut 2003; 53: 416-9. 31.
Fattovich
G: Natural history of Hepatitis B. EASL International Consensus Conference
on Hepatits B. Program and Manuscripts,
Geneva13- 14 Septembar 2002; 47-62. 32.
Puoti
M, Magnini A, Stati T et al: Clinical,
histologic, and virological features of hepatitis C
virus carriers with persistently normal or
abnormal aminotransferase levels. Hepatology
1995; 21: 285-90. 33.
Stanley
AJ, Haydon GH, Piris J et al: Assessment of liver histology in patients with hepatits
C and normal transaminase levels. Eur J
Gastroenterol Hepatol 1996; 8: 869-72. 34.
Pawlotsky
JM: Use and interpretation of virological tests for hepatitis C. Hepatology 2002;
36: S65-S73. 35.
Poynard
T, Bedossa P, Opolon P: Natural history of liver fibrosis progression in
patients with chronic hepatitis C: the OBSVIRC,
METAVIR, CLINIVIR, and DOSVIRC groups. Lancet
1997; 349: 825-32. 36.
Afdhal
NH: Diagnosing Fibrosis in Hepatitis C: Is the Pendulum Swinging From Biopsy to
Blood Tests? Hepatology 2003; 37: 972-4. 37.
Fontana
RJ, Lok ASF: Noninvasive Monitoring of Patients With Chronic Hepatitis C.
Hepatology 2002; 36: S57-S64. |