|
|
Alimentary
tract and pancreas Alimentarni
trakt i pankreas |
||
|
1Dragan
Sagi}, 2Vojislav
N. Peri{i}, 3Bo`ina
Radevi}, 2Mira
Petrovi} 1Department
of Radiology, Institute for Cardiovascular
Diseases Dedinje, 3Department
of Surgery, Institute for Cardiovascular
Diseases Dedinje, 2University
Children,s Hospital, Belgrade. |
ARCH
GASTROENTEROHEPATOL 2003; 22 (No 1 - 2): 12 – 17 Images
in gastroenterology and hepatology Wall-stent
relieve of obstructed
distal splenorenal shunt Osloba|anje
opstrukcije distalnog spleno-renalnog
{anta "wall-stentom" (
accepted May 15th, 2003 ) |
||
|
. |
Twelve-year old boy was admitted to the University Childrenís Hospital, Belgrade for further assessment of hemathemesis, splenomegaly and hematological indices of hypersplenism. At the age of 5-year he was diagnosed as having portal hypertension due to portal vein cavernoma. At that time he bled from the oesophageal varices. Spleen was grossly enlarged, laboatory investigations demonstrated normal liver function tests, leukopenia and trombocytopenia. He successfully undervent selective distal spleno-renal shunt and partial splenic resection by one of us (BR). After operation quick and complete variceal dissapearance,
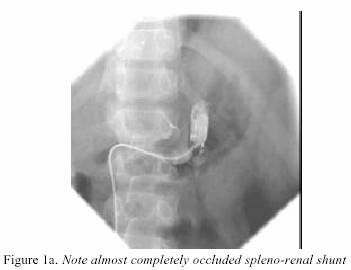
normalisation of hematological indices, and increased growth vlocity were recorded. At admission spleen was palpable 2 cm below the left costal margin. WBC count was 2.7, trombocytes were 67. Upper GI endoscopy demonstrated oesophageal varives of grade III. After femoral vein puncture catheter was introduced via renal vein into the splenic vein. Angiography
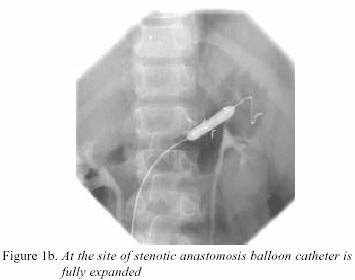
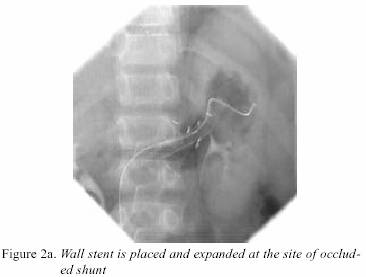
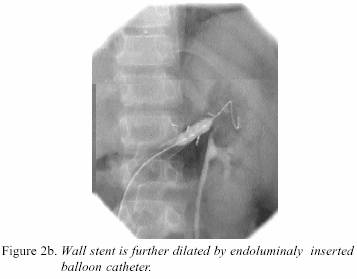
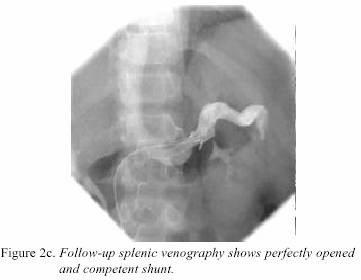
demonstrated almost completely obstructed spleno-renal shunt. Figure 1. Baloon dilatation (balloon caliber: 8mm) of stenotic anastomisis was unsuccessful. Then Wall stent of 9 mm in diameter was placed throught the narrowed shunt and further balloon dilated up to the caliber of 10 mm. Figure 2. This led to full obstruction relieve and reestablishment of shunt patency. Next day oesophagogastroduoenoscopy demonstrated complete varical dissapearance; laboratory analyses showed normalisation of WBC and platelet count. Comment: We alredy
demonstrated that the majority of children and adults with portal hypertension who underwent decompressive shunt surgery has been experiencing prolonged variceal decompression and full relieve of hematological abnormalities due to hypersplenism (1,2). We also demonstrated that compromised spleno-renal shunt was possible to dilate by percutaneous balloon angioplasty with permanent full variceal decompression and hematological remission (3). This case further expand the therapeutical options in controlling failed porto-systemic shunts, eg. spleno-renal anastomosis. According to our knowledge we are the first to demonstrate that in children with obstructed
porto-systemic shunts and fully blown picture of portal hypertension Wall stent dilation of compromised spleno-renal shunt may led to full relieve of clinical and laboratory complications due to potla hypertension. This further imply the necessity for regular "shunt
surveillance" by Doppler ultrasound in dagnosing early signs of shunt shunt incopetence.
|
||
|
|
|||
|
|
|
||
|
|
REFERENCES: 1.
Perišic VN, Radevic B, Sagic
D, Perišic D. Management of eextrahepatic portal
hypertension in children. Arch Gastroenterohepatol
2000; 19:90-3. |
2.
Ješic
R, Radevic B, Sagic D, Tomic D, Krstic M, Aleksic T, Cvejic T, Bulat V,
Šarenac R, Culafic Dj, Bulajic M. The significance of shunt surgery in treatment of portal hypertension. Arch Gastroenterohepatol 2001; 20: 10-3. |
3.
Perisic
VN, Grujicic S, Sagic D, Radevic B, Bojic M. Balloon dilatation of occluded spleno-renal shunt. J Pediatr Gastroenterol
Nutrition 1997; 25: 104-6. |